Learning Outcomes
After this course, participants will be able to:
- Compare and contrast current and emerging wireless hearing aid technology in terms of functionality and end user benefits.
- Describe how these solutions can improve patient satisfaction above and beyond the use of hearing aids alone.
- Explain how to select the appropriate wireless solutions based upon end user needs.
A Brief History of Wireless
To begin, we will look at a brief history of wireless technologies from the end user’s perspective. What does the term “wireless” mean for patients? Anecdotally, I'll share a quick story with you. I fit my father with hearing aids about five years ago. In conversation, I told him that at ReSound, we were working on this wireless hearing aid with fantastic new features. He looked at me quizzically, and asked, "Haven't hearing aids been wireless since the 1970’s?"
His statement was a bit of an eye opener to me. Often, the words that we use mean different things to different people. He was thinking about the body-worn devices from years ago, where the ear piece was connected to the amplifier through a large cable wire. In his mind, he couldn’t see what the big deal was about “wireless” hearing aids. As hearing care professionals, it is important for us to be mindful of the fact that our patients may need to be guided along the way. We can’t assume that they know what we are talking about, and we may need to define and explain new technology. In this case, the word “wireless” should be clarified and defined as the transmission of information without the use of an electrical conductor (i.e., wires). Unlike devices of the past, our use of the word wireless encompasses things like connectivity to accessory devices, or communication between the two instruments the patient is wearing.
This idea of wireless technology is not new. The use of telecoils and induction loops are a form of wireless transmission. When you think about the cable that lines the room, the magnetic field created by the cable, and how that sends sound into the hearing instrument –it is very much a wireless-type paradigm. Another early method of wireless transmission includes infrared systems, such as TV ears, and line-of-sight connections between some form of accessory device and the earpiece. Additionally, and still in use today, is the concept of FM systems. Last but not least, we also have things like hearing aid remote controls. Although this connectivity has been around for quite some time, many consumers (like my father) are unaware of this technology and all the potential benefits.
Overview of Recent Wireless Technologies
Within the last several years, many wireless technological advances have occurred within the hearing aid industry. These advances include the concept of near field magnetic induction, followed by Bluetooth (i.e., radio frequency transmissions, or RF), and other proprietary radio frequency transmissions.
Near Field Magnetic Induction (NFMI)
Wireless systems based on NFMI started to come into play around 2005-2007. NFMI systems work quite well and deliver some good benefits for patients. One use case is that of a patient wanting to listen to their TV wirelessly through their NFMI-equipped hearing aids (Figure 1). Note that if the user’s TV (or other audio source) were not Bluetooth enabled, they would have to first hook up a device to their TV in order to send a Bluetooth signal to the gateway device.
First, you have the TV (your signal of interest); the output from the TV is converted (usually via a converter box) from an analog signal into a Bluetooth signal, which can be transmitted by a radio antenna. Then, the Bluetooth signal is picked up on the other end by the gateway device (e.g., the streamer that’s worn around the neck of the end user). Finally, the signal is converted by the gateway device into an NFMI signal, and sent to the user’s hearing instruments.

Figure 1. Wireless systems based on NFMI combined with Bluetooth (RF).
Since these transmissions are sent via magnetic induction, this is very similar to the type of technology used in a telecoil. It turns the signal into something that can be used by a telecoil, which is then received by a specific antenna within the hearing instruments, and finally changed into an acoustic signal that can be perceived by the end user. The NFMI part of the system contains the transmission energy within a localized magnetic field. This type of transmission is referred to as “near-field transmission” (up to 1 meter). The carrier frequency is generally 10-14MHz. It's a little bit of a different streaming protocol than would be used for an induction loop, since the frequency is so much higher, but yet it still operates using the same principles.
Bluetooth
As a bit of trivia, Bluetooth was named for an ancient king of Denmark who was known as Harold the Bluetooth. His claim to fame was that he united some of the warring factions of Scandinavia. The idea of having a wireless standard called Bluetooth is built upon this desire of having many different pieces of technology being able to “unite, so that they can communicate with each other and share information.
One of the things that has changed in the last couple of years is the way that the TV device and the gateway device communicate with each other: using a Bluetooth transmission frequency. In the past, they may have used another type of proprietary radio frequency. Now, Bluetooth is combined within the gateway device and the TV streamer.
Within about the past five years or so, the term “Bluetooth” has been used in a bit broader sense of the word. Bluetooth is an open standard for wireless communication. Currently, there are nearly 12,000 different products available that use Bluetooth. There are products that can be used, purchased off the shelf, and integrated to be able to communicate with each other. The protocols for Bluetooth must be broad and flexible to accommodate all these different uses.
Typically, we think of Bluetooth as existing in the same frequency region as 2.4 GHz. In reality, Bluetooth uses about 79 frequencies spread out across that 2.4 GHz range. Keep in mind that Bluetooth transmission uses a lot of computational power resources to operate, for which a hearing aid battery isn't a good power source. It is important for an end user to know is that the 2.4 GHz Bluetooth used in hearing instruments today, is not the same as the Bluetooth used to connect your phone to the car, and things of that nature. The power resources needed to drive those technologies are far too great than for something that could be operated by a hearing instrument battery. It's simply not feasible for the direct implementation of Bluetooth within a hearing instrument based on the power requirement.
This lack of battery power is one of the reasons why Bluetooth is being used in some of the streaming technologies. Those devices are remarkably larger than a hearing instrument. A larger device includes a larger battery, resulting in more power that can be used to drive the Bluetooth protocols.
Earlier versions of these different Bluetooth protocols for audio streaming introduced a delay (latency) that is unacceptable for television viewing, because of the mismatch between the audio and visual signals. Bluetooth-based systems that stream audio use the Advanced Audio Distribution Profile (A2DP). The latency for this protocol exceeds 40 milliseconds, and is commonly up to 125 milliseconds, depending on the audio compression technique that is used.
Think about using Bluetooth when you are driving in the car and you want to be hands-free. You are watching the road, and not looking at a visual display. Therefore, you don’t have to worry about the audio being synced with something visual. If any delay occurs, your process of communication will not be too disrupted. On the other hand, for hearing aid applications where there is an audio signal along with a visual element (e.g., when streaming from a TV or to someone wearing a remote microphone a couple of yards away), that latency becomes a major problem. In addition, you have the combinations of streamed sounds along with amplified sounds and the resulting lip-sync problems. On top of that, if you are watching a TV program along with a person who's streaming from the TV, they might hear an overlap of sound where there's a tremendous amount of echo that will be built into it based on these long latencies. Even some of the very small delays, though they're not consciously perceived, will cause a mismatch between audio and visual signals. We need to take that into account when designing wireless systems of the future.
The following graph (Figure 2) is a visual schematic of the way that these delays work. A KEMAR mannequin was used to take these measurements in one of our electroacoustic labs, using some of the early wireless systems that were available on the market.
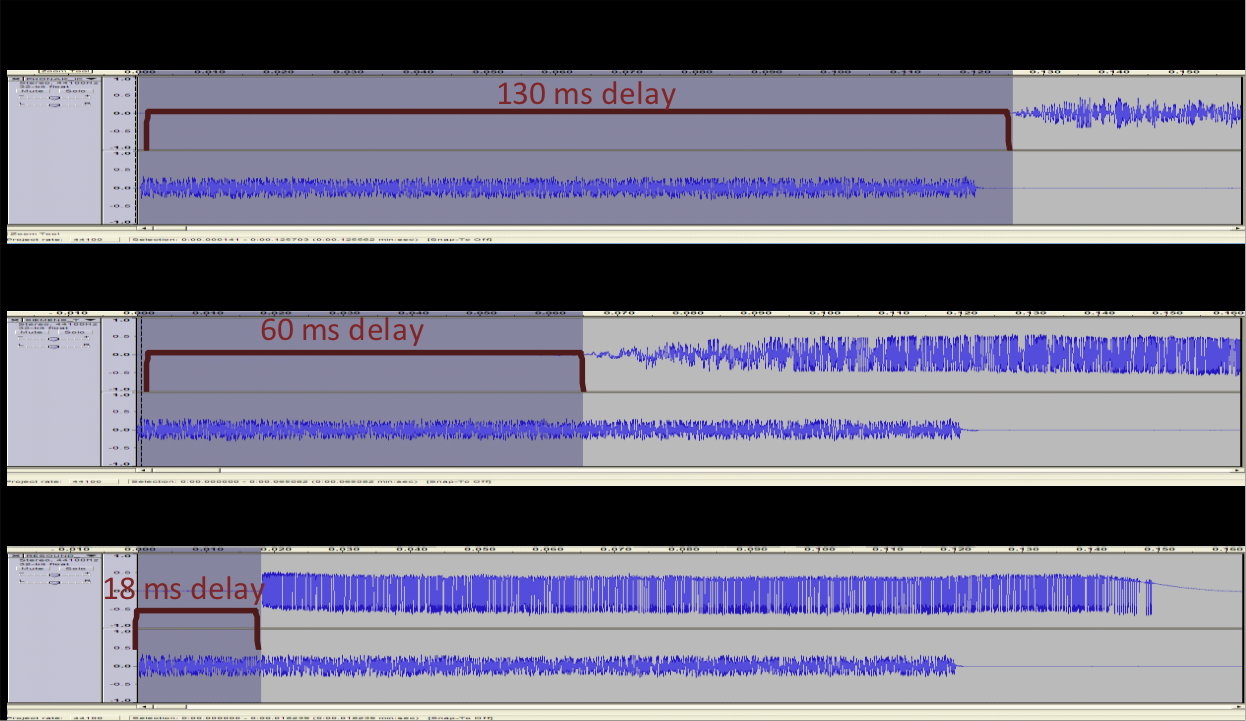
Figure 2. Bluetooth audio delay.
This is a visual representation of the transmission of a short broadband signal. The top broadband signal is just shy of 130 milliseconds (ms) in length. What you're seeing is the transmission of the original signal as measured in a coupler. Then, 130 ms later is when the stream signal came through. If you were to listen to this, this would sound like “shh---shh” where there was an audible tiny gap between when the acoustic signal arrived and when the stream signal arrived. This would be a significant delay that would be very perceptible by most individuals.
Some of the later versions of NFMI technologies were effective in shortening that delay, reducing it down to 60 ms, which would still be fairly perceptible to most end users. The signal in the middle of Figure 2 is a long running signal about 115-120 ms, and the stream signal coming in on top of it. Again, an audible and perceptible delay. If you want to think about an example for it, think of the sound of the guitar from some of the old Elvis recordings back in the 1950’s. We call that a slap-back delay, where it would just make a sound and then a couple of seconds later you hear that sound again. It adds a tinny, metallic quality to it.
The final signal in Figure 2 is a sample of where we are going with the Bluetooth audio delay. Currently, there is an 18 ms delay with the more recent wireless devices. This is one of the benefits of not having to use a gateway device: that the delay can be shortened. This delay tends to go relatively unnoticed. It's usually around the 30 ms mark where the perceivable difference in delay starts to diminish. Over the next several years with improvements in technology, this gap will likely be closed even more. Ideally, it would be great to get it down to the vicinity of 6 ms. At any rate, the delay has been steadily decreasing over time.
Pros and Cons – Wireless Systems Based on NFMI Combined with Bluetooth. A little bit of background now on Bluetooth itself, the way the Bluetooth works, and the previous near-field magnetic induction type strategies, etc. I think when we start to look at advantages and drawbacks for end users, there are some items to keep in mind when choosing different systems that best suit our patients. In terms of advantages, NFMI systems are fairly easy to implement. There are off-the-shelf radio frequency chips that can simply be purchased and plugged in. From a product development standpoint, they are easy to use. NFMI is time-tested technology, strong, robust, and has a longer battery life, due to low current drain on hearing instruments; it's set on the third-party streamer. Many of these devices are rechargeable. In terms of drawbacks, the transmission distance is very short. On average, the user needs to be within one meter in order to be able to receive the broadcast transmission from the gateway device. Due to this short distance, the gateway device typically needs to be worn around the neck. It is an extra piece of equipment, so it adds a certain amount of extra complexity. Historically, sound quality can be affected by the orientation of the gateway device, as well as the hearing aid receiver coil. There can be delays that are introduced by the relay component. This is one of those situations when the gateway device isn't there (i.e., when you cut out the middle man), you can achieve better speed and less latency.
Proprietary Radio Frequency Systems
In Figure 3, you can see the wireless systems based on proprietary radio frequency. You'll notice I've used pictures of ReSound accessories and hearing instruments. This could be the same kind of model used for the 900 MHz streaming protocol in the US, and the 868 MHz protocol for places in Europe and around the world. It looks very similar to the schematic I showed earlier on NFMI. The main difference is that the signal starts from the TV, goes to the A/D converter, into the TV streamer box. It is then sent directly to the hearing instruments, decoded, and transmitted into an acoustic signal by the hearing instruments themselves.

Figure 3. Wireless systems based on proprietary radio frequency.
This is a direct radio transmission. There are different modulation components that go into radio systems, regardless of what you're transmitting (e.g., AM, FM, and pulse width radios). The antenna size and the antenna orientation is very important in both the transmission and reception of the wireless signal.
Let me give you an example. A proprietary radio frequency system uses a radio to generate an electrical wave. The antenna on each end is used to both transmit the signal as well as receive the signal. In these types of systems, all of the transmission energy is designed to radiate into free space. This type of transmission is referred to as “far-field.” Unlike near-field magnetic induction, the antenna is transmitting signals and they are making patterns that generate out in a radiated direction. These signals will ultimately be picked up by the receiver on the other end. These fall into different types of frequency bandwidths. We use ISM, industrial, scientific, and medical frequency bands to categorize and code these frequencies. Hearing instruments today use 900 MHz in the U.S., Greenland, and some of the Eastern Pacific Islands; 868 MHz in the European union; and 2.4 GHz is available for global use within that ISM band.
Keep in mind that these bandwidths have been set aside and reserved for specific applications. For example, microwave ovens occupy a very specific place within the ISM bandwidth. They are designed to work within specific frequency regions to make sure that they don’t cross over and interfere with other gadgets. The microwave oven would be considered more of an industrial appliance. Examples of scientific and medical frequency bandwidth would include MRI machines and equipment of that nature. If some of these different wireless signals were to interact with each other, it could be very detrimental. That’s why they tell you to turn off all cell phones and similar devices when you fly on airplanes. They have to make sure that these two signals won't interfere with each other, because communication errors could occur, resulting in major safety issues. There must be safeguards in place that are designed to mitigate this kind of interference.
This is a table of all the different ISM bandwidths as defined by the International Telecommunications Union (ITU-R) for radio communication (Figure 4). Higher frequency transmission allows for greater data transmission. A trade off exists between amount of data transferred and current consumption. In the U.S., this is one of the reasons why we see some variation in the 900 MHz use across different arenas. This is approved for use in the U.S., but abroad you don’t see widespread use. There are specific situations where you obtain approval. The frequency range 2.4 GHz is broadly accepted. One of the reasons why Bluetooth exists in that range is because it's a broad range where different frequencies can be used for radio transmission.
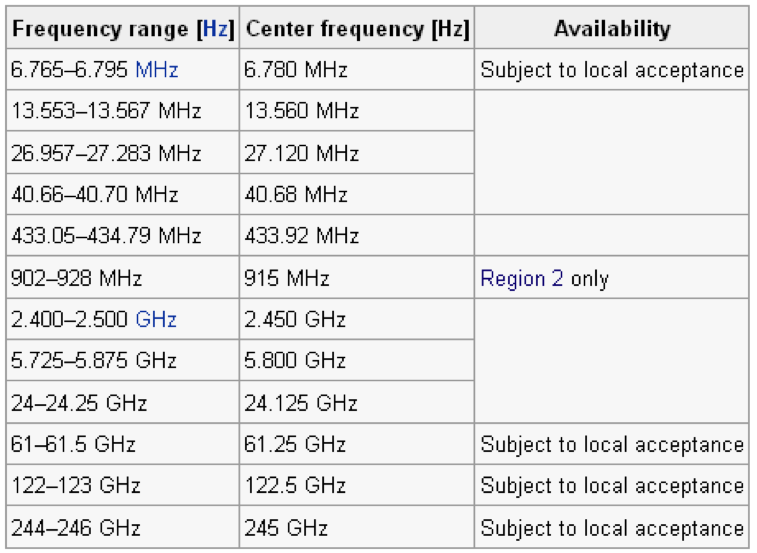
Figure 4. ISM Bandwidths.
ISM Transmission. From a patient-centered perspective, our devices are designed to be error tolerant so that you don’t get interference. These ISM bands can become congested with all sorts of different audio and data applications. The question arises: How do we make sure that data is transferred reliably? There are two main techniques: spread spectrum frequency hopping and point-to-point data transmission.
Spread spectrum frequency hopping is based on the notion that we are transmitting a signal on many different frequencies within the vicinity of the 2.4 GHz frequency band. The signal won't always be trying to hit that single 2.4 GHz frequency; it might “hop” between different frequency ranges (e.g., from 2.39, to 2.42, to 2.35, etc.). Imagine if you're playing a piano keyboard and only trying to get someone to hear one specific note. In essence, what we do is play some of the other frequencies or other pitches right around that note, in order to make sure that it gets transmitted. The idea with a pairing process is to ensure that we have point-to-point data transmission. That’s a major component of what makes all this wireless technology work. As a side note, there was a program that I watched recently that indicated that the actress Hedy Lamarr was one of the primary inventors and early investigators on the idea of spread spectrum frequency hopping.
Why is it important for you to know about frequency hopping? From a patient standpoint, it helps to troubleshoot when they are having issues. If they lose connection sometimes, ask them if there are other wireless transmissions going on in their environment. It might be their wireless network, or some other kind of transmission device that is interfering. Help them figure out what is close to the device. Does it drop off when a certain piece of equipment is running (like when the microwave is on, or when they are printing a document)? Those are some of the issues that a novice end-user might experience, and they may not possess the knowledge or technical background to understand how these systems work. It is a benefit that the patient is no longer is required to wear the gateway device around their neck, but they need to be aware that there may be an opportunity for issues if the wireless network gets congested.
As discussed earlier, NFMI wireless systems have a limited range of about three feet. It is physically impossible for conventional wireless to transmit more than three feet without a big interim device. This will never change. In contrast, the robustness of the signal based on proprietary radio frequency (RF) allows our 2.4 GHz to transmit 10 times further than conventional wireless. This schematic (Figure 5) highlights the potential transmission range (approximately 10 meters / 30 feet). When there are other surfaces around the two devices transmitting and receiving, there can be a lot of radio reflections, in the same way that there are acoustic reflections. This range of 30 feet is fairly theoretical and is also fairly conservative. You can see some transmissions of even more than 30 feet. Granted, when you get outside and there are fewer reflections, that 10-meter or 30-foot range is probably a bit more accurate across the board.
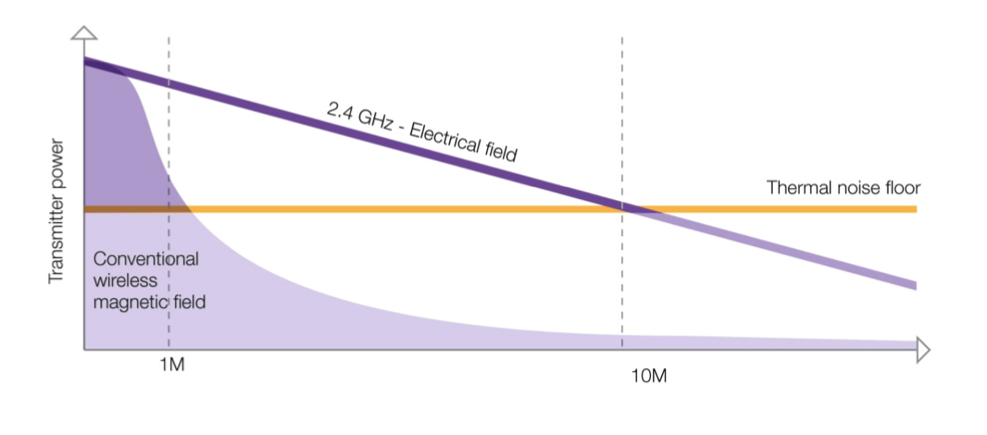
Figure 5. 2.4 GHz transmission range. This is an illustration only; not a representation of sound but of the electrical currents on which sound is carried.
Where are We Going?
Bluetooth Smart (Low Energy)
Bluetooth Smart is also known as Bluetooth Low Energy, Bluetooth LE, Bluetooth 4.0. All these terms are considered to be synonymous. Essentially, they are ways of taking that original Bluetooth protocol and optimizing it for small devices that don’t have large batteries in them. For the most part, these are sensor-type devices. Think about gadgets such as FitBits and Apple watches: they don’t require much power and do not require the need to stream audio. Having the audio part separated out makes for a much more efficient strategy for streaming.
New Global Standard
This Bluetooth LE technology has opened up some new doors. According to a press release in March of 2014, the European Hearing Instrument Manufacturers Association (EHIMA) had announced a new partnership with the Bluetooth Special Interest Group (SIG). Cooperatively, these two groups aim to develop a new Bluetooth standard for hearing aids. I have no inside knowledge about how far along they are in these efforts, but there are definitely meetings going on aimed at creating this new global standard for hearing aids with Bluetooth connectivity. Because of the optimized manner with which Bluetooth LE technology works, it is ideally suited to be used on a small scale for devices with small batteries, such as hearing aids.
The Future of Wireless Connectivity
Made for iPhone
It is no secret that the future of wireless connectivity involves smart phones, and the use of features like direct connectivity to hearing aids for phone calls, as well as apps, internet access, etc. The made-for-iPhone (MFI) hearing aids made a significant impact on the development of wireless hearing aids. In essence, made-for-iPhone hearing aids mean that a direct stereo audio and data stream is made possible between the hearing aids and Apple devices, such as iPhones and iPod Touch. Streaming sounds directly to hearing instruments is an excellent way to increase audibility and word recognition during phone calls or FaceTime. You can now give your patients endless possibilities on equal terms, and in some cases even better, than normal hearing, as hearing aids are converted into 24/7 wireless stereo headphones requiring no additional hardware. This also means that with MFI, you have the opportunity to forever free the end user from the stigma of wearing complicated neck loop streamers around their neck.
In addition to the improved wireless streaming features, there are new applications that allow a user to fine tune their hearing instruments. These features are opening up a lot of doors in terms of patient engagement, because the display offers a lot of “visual real estate” (Figure 6).
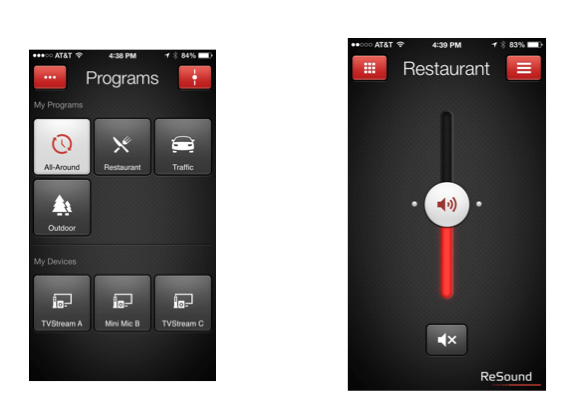
Figure 6. Updates to user interface display.
This display allows users to better understand what kinds of possibilities they have with being able to change and adjust their devices based on their surroundings. Users did previously have access to make changes, but it wasn’t as visually stimulating or intuitive. These improvements to the interface, along with other updates that have been made, are changing the paradigm for how hearing instruments are worn and used, both now and for the future.
There are also some other great features, such as Find My Hearing Aid, the ability to geotag locations and attach settings to a specific place, and the option to further personalize the hearing aids.
Wireless Fitting
So far, what we have covered has been end user focused and very technological. With regard to wireless fitting, there are other great benefits. Wireless transmission is not limited to streaming; data transmission is also quite common such as with a remote control or for wireless fittings.
Recently, I was working with an individual on some adjustments to their hearing aids. However, we were not in my office. I was traveling on a work trip and we were sitting in a restaurant and I was able to do the fine tuning in the middle of the restaurant. With a wireless connection, I was able to sit down, make the adjustments, and have the person experience it in real time. No one sitting in the restaurant had any awareness of what we were doing. For all they knew, I was giving him financial advice and I was using my laptop.
These types of wireless fittings open up a huge new avenue for making changes in unconventional environments or settings that are problematic for the patient. You now have the technology that gives you the opportunity to easily make adjustments outside of your office.
Wireless Ear-to-Ear Signal Processing
One main function of wireless technology is, of course, Ear-to-Ear signal processing that allows improvements in directionality/hearing in noise, localization, feedback cancellation, and phone communication, as well as in ease of use as you can synchronize the settings between the two ears. Refer to your handout for a few further details in each of these areas. Figure 7 is entitled “Think System” as when it comes to wireless technology, you are working with a system rather than each component in isolation

Figure 7. Think System.
Research and Market Analysis
Two fundamental questions that I'll pose to the audience today are:
- Are these technologies making any kind of a difference?
- Why do we think these technologies will make a difference?
With that, let me give you some background on research that I've used to prepare for this talk. Before we had our 2.4 GHz wireless system, we did some market analysis to determine what the needs were for both end users and fitters. My colleagues Groth and Anthonsen published an article in the Hearing Review in 2010. It describes results of a study that indicated that accessories were included in less than 30 percent of fittings with hearing instruments that had wireless features. There were a few outliers who were using them most of the time. These days it seems to be a little bit more (30-50%).
Another key takeaway from this study was that wireless hearing instruments were generally fit to younger patients than non-wireless ones. Wireless usage goes down as age increases, non-wireless goes up as age increases. There is a bit of a stereotype that we have to be cautious in using anything hi-tech with the older generation, and we tend to only offer wireless to our young, tech-savvy patients. I believe there is a missed opportunity there. We should not underestimate the technical capabilities of the older generation.
Prior to 2010 and the introduction of 2.4 GHz, we knew that the wireless accessories available at that time did what they claimed they were going to do. They overcame problems with distance, excessive background noise, and poor room acoustics. Unfortunately, they had problems such as latency, which resulted in issues with sound quality, and the extra gateway device was another piece of equipment that the end user had to use. Finally, hearing care practitioners were only using accessories when end users stated specifically that they had a problem with the TV, or when they demonstrated some form of familiarity with technology.
In 2014, Smith and Davis published an article in the International Journal of Audiology on the benefits of Bluetooth accessories with hearing aids. They had a cohort of subjects who were fit both with hearing aids alone, and then also hearing aids plus accessories. Then they measured the benefit in the two different conditions using the Glasgow Hearing Aid Benefit Profile (similar to the AFAB in the U.S.). In comparing the two conditions, they found that the use didn’t change significantly, but there was an increase in residual benefit and residual satisfaction when the hearing aids plus accessories were used. There was increased benefit when the whole system is being used together, not just with the device itself.
I specifically mentioned some of the aging aspects of the 2010 study, because of the findings from this newer article. Smith and Davis highlighted in their study the positive correlation between age and benefit. In other words, older patients had higher benefit scores. Essentially, the older the patients, the greater the benefit they received from using these technologies. This study suggests that we need to reevaluate our thought processes and change our recommendations when fitting older patients.
There was also a significant negative correlation between the hearing threshold levels and the benefit profile. In other words, the patients who had lower levels of hearing loss received a more benefit from the instruments with the accessories. This correlation resonated with me very strongly because of my experience with fitting the test devices, and being on the leading edge of technology before it goes into the real world. I have had a couple of patients with thresholds of around 25 to 30 dB across the board. We tend to think of those people as potentially benefiting from a hearing aid, but they might not really get that much from it.
With one patient in particular, I was demonstrating a remote microphone. As I walked out of the room away from her and down the hall, I continued to talk to her. The patient was sitting in the room with one of my colleagues who had normal hearing. The patient looked at my colleague and said in awe, "Oh, I've heard everything he says as he's walked down the hallway," whereas my colleague hadn’t heard anything that I said. You could see the reaction on her face where she thought, "Wow. I'm hearing things that other people aren’t." In cases using accessory technologies, perhaps the cure is no longer worse than the disease. We're able to give people solutions and options that open up a wide range of opportunities for the future. As taken directly from the Smith et al article: “It is clear that patients using hearing aids report additional benefits from using Bluetooth accessories.”
Researchers highlight the need for training between clinician and end users. We have to take steps to bring these technologies in earlier and try to make them a more accessible to patients, and make them easy to use.
Summary
What can be done to bring this “think system” mentality into your daily routine? I'm an advocate for investigating the livability of these devices for yourselves. Get a set of hearing instruments, use them, learn about them, figure out how they work, and analyze what their strengths and weaknesses are. Whenever I test the devices here in our clinic, I have a set that I use myself to get a feel for everything that they can and cannot do. That helps me raise my level of expertise so that I can effectively work with patients as problems arise. Next, I recommend that you augment your intake forms to include questions about technology attitudes and opportunities for situational use. This will prevent us from making the mistake of pigeonholing certain patients into groups labeled “they will use this” or “they won't use that.” Use demonstration to illustrate the concept and, use contextual training to make the use relevant. Finally, begin to develop a “clinical narrative” to ensure the benefits provided by these technologies are communicated throughout the hearing care journey.
If you have any questions, feel free to reach out to me via email - shallenbeck@gnresound.com.
Questions and Answers
This idea of contextual training, what does that mean?
Imagine if a patient comes in and you're teaching them how to use a set of hearing instruments or an accessory. It's very easy to just go through the steps and show them where the “on” button is, how to use the volume control, do this, that, and the other thing. The idea of contextual training is to turn the training over to the patient, and have them tell you how they think they're going to use it. Then you can get in there and shortcut some of the things that will or will not work for them when they get out into the environment.
Example, instead of saying “when a phone call comes in, press this button to answer it,” call them and let them answer the phone and go through that whole process themselves. It's much more hands on, much more tangible, and much more easy for the patient to take up.
What is BLE?
In brief, it's Bluetooth low energy, synonymous with things like Bluetooth smart, Bluetooth 4.0. Bluetooth low energy is just a different type of Bluetooth protocol that allows for more efficient transmission at lower power levels.
Which uses more power, audio or control data?
Typically, the audio is going to require much more power than the control data because the control data consists of much smaller data packets. They're just sending a piece of information. It's a very discrete and small bit of information that changes something about the hearing instrument versus the audio data. Imagine it like this: it would be the difference of downloading a song from the internet versus using your remote control to turn up the volume on the TV. Two much different power requirement needs based on the amount of data that’s being transmitted, small data packets versus very large audio packets.
Is power consumption the main barrier for direct Bluetooth?
Yes. I would say it's probably the main barrier for the direct Bluetooth link. This is especially true with Bluetooth of years past when you're talking about the full protocol that’s used in those very computational and very large data packets.
References
Groth, J., & Peterson, F. (2010). Fewer wires, less complexity, and more connections: The new challenge for wireless hearing instruments. Hearing Review, 17(6), 28-36.
Smith, P., & Davis, A. (2014). The benefits of using Bluetooth accessories with hearing aids. International Journal of Audiology, 53(10), 770-3. doi: 10.3109/14992027.2014.941075
Citation
Hallenbeck, S. (2016, August). Wireless technology: Where have we been? Where are we now? Where are we going? AudiologyOnline, Article 17925. Retrieved from https://www.audiologyonline.com

