
Abstract
Importance: Tinnitus is a common problem for millions of individuals and can cause sleep disturbances and poor quality of life.
Objective: To assess whether high frequency directed audio, using ultrasonic technology delivered via HSS reduces the perception of tinnitus in subjects with chronic, non-pulsatile tinnitus.
Study Design: Pre- and post-intervention clinical outcomes study.
Patients: Eleven adult patients with chronic, non-pulsatile tinnitus. Four subjects had unilateral chronic tinnitus and seven patients had bilateral chronic tinnitus.
Intervention(s): Subjects were exposed to a quiet environment for 5 minutes to establish their tinnitus baseline and complete the Tinnitus Handicap Inventory (THI) and a Visual Analog Scale (VAS) for tinnitus loudness (VAS-L) and annoyance (VAS-A). Subjects, in consultation with the investigator, selected from a choice of customized acoustic stimuli available on the HyperSound Tinnitus Application (HS Tinnitus App). The HyperSound audio system was tuned by the investigator to the patient’s audiogram using a standard fitting algorithm. Subjects, with consultation from the investigator, then used the HS Tinnitus App to adjust equalizer (EQ) settings to fine tune the frequency response of the HyperSound system audio output and the volume to their personal preference where they felt they received the most masking of their tinnitus. Subjects were then exposed to the customized acoustic stimulus for a duration of 60 minutes. After 60 minutes, subjects completed the Tinnitus Handicap Inventory and a Visual Analog Scale for tinnitus loudness and annoyance while in the customized acoustic stimulus.
Main Outcome Measure: 100 point validated Visual Analog Scale for tinnitus loudness and annoyance pre- and post-exposure to HyperSound.
Results: Highly significant reduction in tinnitus loudness and annoyance was observed in all subjects during exposure to a customized acoustic stimulus delivered with high frequency directed audio. The mean VAS-L scores decreased by 61% from a pre-exposure mean score of 59.6 to a post-exposure mean score of 23.5 (p=0.000053). The mean VAS-A scores decreased by 54% from a pre-exposure mean score of 64.3 to a post-exposure mean score of 29.5 (p=0.000068).
Conclusions: Delivery of a customized acoustic stimulus via high frequency directed audio using ultrasound technology demonstrates dramatic reduction in tinnitus loudness and annoyance during exposure to the stimulus. This technology may have significant implication for management of chronic, non-pulsatile tinnitus.
Introduction
Tinnitus is a condition whereby sound is heard without an external acoustic stimulus. It is often described as a constant tone (ringing), hissing, or roaring. Prevalence studies in western Europe and the USA have shown rates as high as 15% in the adult population (Baguley, McFerran, & Hall, 2013) with an estimated 20 million Americans that suffer from tinnitus. Researchers believe there are four primary effects of tinnitus on daily life: 1) thought and emotions, 2) hearing, 3) sleep, and 4) concentration. Tinnitus is a significant cause of diminished quality of life as well as depression, anxiety, insomnia, fatigue, and difficulty with concentration. Each person is affected differently by tinnitus, which complicates management. The condition can occur from a variety of sources including disease and hearing damage, and can range in intensity from mildly annoying to completely debilitating (Claussen & Pandey, 2009).
An integral part of tinnitus therapy involves stimulus from an external audio source. Along with psychological counselling, sound therapy is recommended per clinical guidelines from the American Medical Association (Walker, Cifu, & Gluth, 2016) and the American Academy of Audiology (2001). Sound therapy can vary from broadband noise to specific tones (Tyler, Stocking, Secor, & Slattery, 2014). With sound therapy, many patients experience masking whereby the perceived tinnitus is diminished (Alexander & Schleuning, 1997). Other patients may not experience masking, but do experience relief with the external stimulus.
The HyperSound Audio System (HSS) functions by creating a beam of sufficiently high-intensity ultrasound that demodulates in the air column to form a beam of audible sound. This parametric audio was first hypothesized and demonstrated in the 1960s and 1970s (Westervelt,1963; Berktay & Leahy, 1974; Bennett & Blackstock, 1974). Initially only capable of highly-distorted audio, many years passed before quality audio reproduction could be achieved due to high-speed digital processing. HyperSound, first released in 2015 to improve clarity and speech intelligibility, achieves beams of directed audio using proprietary processing techniques and an advanced capacitive transducer similar to those studied by Rafiq and Wykes (1991), and Ge (1999). One recent study indicated HSS enhances speech understanding in subjects with mild to severe hearing loss (Mehta, Mattson, Seitzman, & Kappus, 2015). For the purposes of the present study, HSS is used to project a beam of masking audio stimulus to a subject with tinnitus.
The effectiveness of the masking greatly increases if the equalization can be tuned for the specific user (Tyler et al., 2014). Tyler and colleagues showed that a patient-specific tone could help 2.7 times more patients when compared to basic noise. There is also some evidence that extremely high frequency sound is a very effective masker (Goldstein, Lenhardt, & Shulman, 2005). In that study, Goldstein and colleagues measured significant tinnitus benefit with a bone-conducted acoustic stimulus using audio frequencies only from 6 kHz to 20 khz, with the bulk of the energy above 10 kHz. These two results make HSS an extremely attractive candidate for producing masking audio. Unlike standard inductive loudspeakers, HSS efficiency increases with frequency and is very effective at producing sound in the highest audible octaves (Westervelt, 1963). For equalization customization, the HSS HyperFit software tool (for professional use only) can adjust baseline equalization. Using the HSS Tinnitus application, a hearing professional and the subject can optimize the equalization even further for maximum effectiveness. In addition, because of the beam-like nature of HyperSound audio, users can receive sound therapy without disturbing other individuals in the same environment, without the need to wear headphones.
Exposure to ultrasound from HyperSound has been extensively evaluated for safety. Exposure for up to two hours has shown no threshold shift nor onset of new otologic symptoms (Mehta, Mattson, Kappus, & Seitzman, 2015). In comparison to ultrasonography or High-Intensity Focused Ultrasound (HIFU), HyperSound delivers less that 1/12,000th of the energy to the body and is within the limits of human safety (Nelson, Fowlkes, Abramowicz, & Church, 2009; Haar & Coussios, 2007; Jewell, Solish, & Desilets, 2011), including standards set by the Occupational Health and Safety Administration (OSHA).
Method
Participants
Participants were eligible for the study if they were age 18 years or older and had chronic non-pulsatile tinnitus, either unilateral or bilateral. Eleven adult patients were deemed eligible. Participants were not eligible for the study if they had cochlear or middle ear implants, wore extended-wear hearing aids, had recent (within one month) or ongoing psychiatric treatment, or had pulsatile tinnitus.
Equipment
All testing was completed at the California Hearing & Balance Center in Carlsbad, California. Participants were seated at approximately 6 feet from the HyperSound audio system that consisted of two emitters and one amplifier. Connected to the amplifier was an Apple iPad Mini running custom software and stimulus content provided by Turtle Beach Corporation to provide tinnitus-specific, adjustable audio content.
Outcome Measures
The primary outcome measured is change in VAS loudness and VAS annoyance, as measured by the Visual Analog Scale for tinnitus. A 100-point VAS for the assessment of chronic tinnitus has been demonstrated to be a reliable and valid measure of tinnitus severity with a minimum clinically identifiable difference (MCID) of 10-15 points (Adamchic, Langguth, Hauptmann, & Tass, 2012).
Horizontal VASs, verbally anchored at the endpoints were used (Torrance, Feeny, & Furlong, 2001). The endpoints were designated as “not audible” and “extremely loud” for the Visual Analog Scale – Loudness. The endpoints for the Visual Analog Scale – Annoyance were designated as “not annoying” and “extremely annoying”. The purpose and use of the VAS was explained to the subjects, and they were told that the scales are used to assess the loudness and annoyance of their tinnitus. If they felt that their tinnitus was extremely loud/annoying, they marked the right side of the scale. If they felt their tinnitus was not audible or not annoying, they put a mark at the left side of the corresponding scale. Subjects marked their impression of intermediate strength of loudness/annoyance somewhere along the VAS length. During analysis, the “not audible/not annoying” endpoint corresponded to 0 and the “extremely loud/extremely annoying” corresponded to 100 with intermediate results rated between 0 – 100.
The Tinnitus Handicap Inventory is a psychometrically robust, validated self-report tinnitus handicap measure that is brief, and easy to administer and interpret (Newman, Jacobson, & Spitzer, 1996) The THI consists of a 25-item questionnaire scored from 0-100. The THI was administered at baseline and post-exposure.
Procedures
After signing an informed consent form, baseline hearing levels were determined by testing pure-tone air conduction thresholds at 250-8000 Hz. This data was used to program a custom equalization curve into the HyperSound amplifier based on pure tone thresholds using the proprietary HyperFit software, which attempts to equalize loudness for average level inputs using the NAL-R formula (Byrne & Dillon, 1986).
Before beginning testing, participants were exposed to a quiet environment for 5 minutes to establish their tinnitus baseline. If the subject used hearing aids, they were removed for the duration of the exposure. Baseline tinnitus levels and handicap were determined using the Tinnitus Handicap Inventory and a Visual Analog Scale for patient reported measurement of subjectively perceived tinnitus loudness and tinnitus annoyance.
Each participant was seated approximately 6 feet away from the HyperSound system and received an Apple Ipad Mini running a custom HyperSound Tinnitus application. This application produced a variety of sounds which included rain, wind, sea hitting rocks, lapping waves, as well as white, pink, and brown noise. Subjects, in consultation with the investigator, could select a sound that they preferred and using the application, adjust equalization in ½ octave bands from 1.5 kHz to 16 kHz (plus additional bands at 10 kHz and 14 kHz) by +/-10 dB. In addition, absolute volume was adjusted on the HyperSound amplifier to the subject’s preference.
After 60 minutes, subjects completed the Tinnitus Handicap Inventory and a Visual Analog Scale for tinnitus loudness and annoyance while in the customized acoustic stimulus.
Statistical Analysis
All patient demographics, hearing loss and tinnitus history, baseline PTA, baseline tympanometry, and other relevant baseline characteristics are presented using standard descriptive statistics. Continuous variables are reported using appropriate measures of dispersion and central tendency (means, medians, ranges and standard deviations).
THI, VAS-L, and VAS-A scores are summarized (means, medians, ranges and standard deviations) and post-exposure was compared to baseline using a two-tailed T-test.
Results
Baseline characteristics for all participants are presented in Table 1. There were six males and five females with a mean age of 59 years. Nine of the participants were of Caucasian descent, one was of African American descent, and one was of Hawaiian/Pacific Islander descent. Mean PTA for the right ear was 29 dB and mean PTA for the left ear was 34 dB.

Table 1. Participant baseline characteristics. PTA = pure tone average; SD = standard deviation.
Tinnitus handicap inventory, loudness and annoyance scores pre- and post-treatment are presented in Table 2. Loudness and annoyance scores were measured using a visual analog scale score from 1 to 100, with the higher number corresponding to a more undesired condition.

Table 2. Tinnitus scores pre- and post-treatment. Tinnitus Handicap Inventory (THI) score does not change significantly with short term treatment. The Visual Analog Scale asks subjects to rate their tinnitus loudness (VAS-L) and tinnitus annoyance (VAS-A) on a scale from 0 to 100. P-values are calculated using a two-tailed t-Test.
Discussion
Subjects reported a decrease in both tinnitus loudness and tinnitus annoyance, reducing from 60 to 23 points and 64 to 29 points respectively (P=0.0005 and P = 0.00007) while in the HyperSound beam with tinnitus sounds playing. This is well above the minimum clinically identifiable difference of 10 to 15 points (Adamchic et al., 2012) Subjects therefore experienced significant tinnitus masking and relief while listening to HyperSound. A survey of THI was conducted after the exposure which did not show a significant difference. This could be due to the limited exposure time studied and could change with future longer-term studies.
Figure 1 shows the audio spectrum of each masking sound provided in the study. This is the maximum volume possible on the system with both HyperFit EQ and HSS Tinnitus App EQ adjusted to max settings (with corresponding gain shown in Figure 1). The final spectrum that the subjects experienced is therefore lower than the one presented and adjusted using the NAL-R prescription using their PTA. Nature sounds were greatly preferred compared to noise with only one out of the 11 subjects selecting white noise. The most popular nature sound was rain with 4 out of 11 selecting this sound as their preference. Rain contains the most high-frequency content compared to other nature sounds provided which is likely the reason it was successful. Most subjects found it unnecessary to adjust equalization via the HS Tinnitus App (n=7) which implies programming the HyperSound system is an effective tuning method for most users.
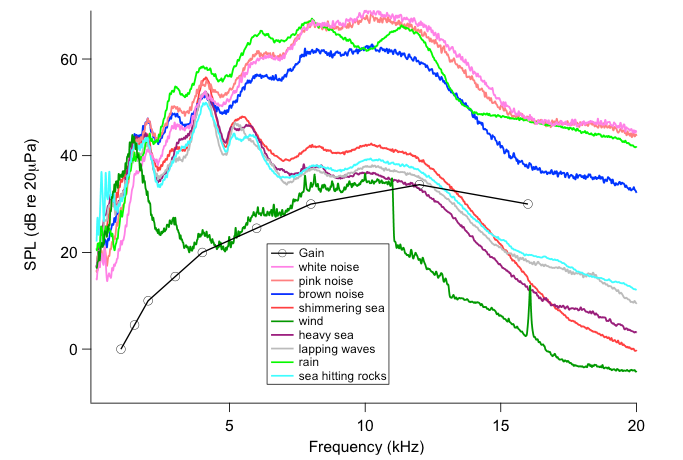
Figure 1. Audio spectrum at 6 feet for various masking sounds at maximum volume and maximum gain settings. The sound is measured using a B&K 4145 1’’ microphone and sampled at 625 kHz to prevent aliasing. The plots represent the average sound pressure level (SPL) for each masking sound. Gain represents the maximum decibel (dB) adjustment possible from HyperFit for a given frequency.
The effectiveness of HyperSound as a tinnitus masker could be due to more than just high-frequency audible sound delivery. Bone-conducted ultrasound can be perceived and has been studied as a potential masker (Nishimura, Nakagawa, Sakaguchi, & Hosoi, 2003; Carrick, Davies, Fielder, & Bihari,1986; Meikle, Edlefsen, & Lay, 1999). This perception of ultrasound does not occur with HyperSound because of lower intensity relative to bone-conduction. However, some ultrasound does reach the inner ear and might provide some benefit (Unpublished data, Laser Vibrometry Studies, Turtle Beach Corporation).
HyperSound creates audible sound by mixing ultrasonic frequencies in the air. Mixing of sound also occurs within the ear, which is typically referred to as “phantom tones” (Barral & Martin, 2012). Using this effect with bone-conducted ultrasound has been shown to aid the profoundly deaf (Nakagawa, Fujiyuki, Okubo, Hotehama, & Kagomiya, 2013). Thanks to the high-velocity yet low-displacement nature of ultrasound, when compared to regular audio, it may be more effective at stimulating difference tones in inner hair cells (Dallos, Billone, Durrant, Wang, & Raynor, 1972).
HyperSound represents a unique solution for tinnitus sound therapy by being an effective, private, sound-delivery system that does not encumber the patient. Traditional masking sounds, especially if they need to be delivered at high volume, are limited to hearing aid-like devices to avoid disturbing others. HyperSound can supply this stimulus in an open room without undue sound leakage. Sleeping, in particular, also poses a problem for wearable devices and is a common aggravating time for tinnitus patients. HyperSound can provide sound therapy for prone users without discomfort and without disturbing others.
As evidenced by the THI results, one hour of exposure was not enough to impact the tinnitus subject’s perceived distress secondary to tinnitus. It was also evident that suppression of tinnitus did not persist once the subject was no longer exposed to the customized sound therapy. Future work includes longer-term exposure, which could improve therapeutic effects and result in long-term inhibition of tinnitus.
Acknowledgments
The research was supported by Turtle Beach Corporation, San Diego, California. The authors would like to thank Brian Taylor, AuD, Senior Director of Clinical Affairs, Turtle Beach Corporation, for suggestions to the manuscript.
References
Adamchic, I., Langguth, B., Hauptmann, C., & Tass, P.A. (2012). Psychometric evaluation of visual analog scale for the assessment of chronic tinnitus. AJA, 21(2), 215-225.
Alexander, J., & Schleuning, R.M. (1997). Use of masking for tinnitus. International Tinnitus Journal, 3(1), 25-29.
American Academy of Audiology. (2001). Position Paper: Audiologic Guidelines fro the Diagnosis and Management of Tinnitus Patients. Audiology Today, 13(2), 23-24.
Baguley, D., McFerran, D., & Hall, D. (2013). Tinnitus. Lancet, 382(9904),1600-07.
Barral, J., & Martin, P. (2012). Phantom tones and supressive masking by active nonlinear oscillation of the hair-cell bundle. PNAS, 109, E1344-E1351.
Bennett, M.B., & Blackstock, D.T. (1974). Parametric array in air. Journal of the Acoustical Society of America, 57(2), 562-568.
Berktay, H.O., & Leahy, D.J. (1974). Farfield performance of parametric transmitters. Journal of the Acoustical Society of America, 55(3), 539-546.
Byrne, D., & Dillon, H. (1986). The Antional Acoustic Laboratories (NAL) new procedure for selecting the gain and frequency response of a hearing aid. Ear & Hearing, 7, 257-265.
Carrick, D.G., Davies, W.M., Fielder, C.P., & Bihari, J. (1986). Low-powered ultrasound in the treatment of tinnitus: A pilot study. Br. J. Audiol., 20(2), 153-155.
Claussen, C-F., & Pandey, A. (2009). Neurootological differentiations in endogenous tinnitus. The International Tinnitus Journal, 15(2), 174-184.
Dallos, P., Billone, M.C., Durrant, J.D., Wang, C., & Raynor, S. (1972). Cochlear inner and outer hair cells: Functional differences. Science, 177(4046), 356-358.
Ge, L.F. (1999). Electrostatic airborne ultrasonic transducers: Modeling and characterization. IEEE Transactions on Ultrasonics, Ferroelectrics, and Frequency Control, 46(5), 1120-7.
Goldstein, B.A., Lenhardt, M.L., & Shulman, A. (2005). Tinnitus improvement with ultra-high-frequency vibration therapy. International Tinnitus Journal, 11(1), 14-22.
Haar, G.T., & Coussios, C. (2007). High intensity focused ultrasound: Physical principles and devices. International Journal of Hyperthermia, 23(2), 89-104.
Jewell, M.L., Solish, N.J., & Desilets, C.S. (2011). Noninvasive body sculpting technologies with an emphasis on high-intensity focused ultrasound. Aesthestic Plastic Surgery, 35(5), 901-912.
Mehta, R.P., Mattson, S., Kappus, B.A., & Seitzman, R.L. (2015). Safety of the HyperSound Audio System in Subject with Normal Hearing. Audiology Research, 5(136), 80-83.
Mehta, R., Mattson, S., & Seitzman, R., & Kappus, B. (2015, August). Speech recognition in the sound field: directed audio vs. conventional speakers. AudiologyOnline, Article 14901. Retrieved from www.audiologyonline.com
Meikle, M.B., Edlefsen, L.L., & Lay, L.W. (1999). Suppression of tinnitus by bone conduction of ultrasound. Poster presented at the Twenty-First Annual Meeting of the Association for Research in Otolaryngology.
Nakagawa, S., Fujiyuki, C., Okubo, Y., Hotehama, T., & Kagomiya, T. (2013). Development of a novel hearing-aid for the profoundly deaf using bone-conducted ultrasonic perception: Evaluation of transposed modulation. Conf Proc IEEE Eng Med Biol Soc., 3574-7. doi: 10.1109/EMBC.2013.6610315
Nelson, T.R., Fowlkes, B., Abramowicz, J.S., & Church, C.C. (2009). Ultrasound biosafety considerations for the practicing sonographer and sonologist. Journal of Ultrasound in Medicine, 28(2), 139-150.
Newman, C.W., Jacobson, G.P., & Spitzer, J.B. (1996). Development of the Tinnitus Handicap Inventory. Arch Otolaryngol Head Neck Surg, 122, 143-8.
Nishimura, T., Nakagawa, S., Sakaguchi, T., & Hosoi, H. (2003). Ultrasonic masker clarifies ultrasonic perception in man. Hearing Research, 175(1-2), 171-177
Occupational Safety and Health Administration. (n.d.). OSHA Technical Manual, Section III: Chapter 5 - Noise. Retrieved from US Department of Labor, Occupational Safety and Health Administration, www.osha.gov
Rafiq, M., & Wykes, C. (1991). The performance of capacitive ultrasonic transducers using v-groved backplates. Meas. Sci. Technol., 2(2), 68.
Torrance, G.W., Feeny, D., & Furlong, W. (2001). Visual analog scales: Do they have a role in the measurement of preferences for health states? Med Decis Making, 21(4), 329-334.
Tyler, R., Stocking, C., Secor, C., & Slattery, W.H.III. (2014). Amplitude modulated S-tones can be superior to noise for tinnitus reduction. American Journal of Audiology, 23, 303-308.
Walker, D.D., Cifu, A.S., & Gluth, M.B. (2016). Clinical practice guideline: Tinnitus. JAMA, 315(20), 2221-2222.
Westervelt, P.J. (1963). Parametric acoustic array. Journal of the Acoustical Society of America, 35(4), 535-537.
Citation
Mehta, R., Mattson, S., & Kappus, B. (2016, September). Treatment of tinnitus using a customized, ultrasonic acoustic stimulus delivered via the HyperSound Audio System. AudiologyOnline, Article 18261. Retrieved from https://www.audiologyonline.com



