Editor’s note: This text-based course is a transcript of the webinar, Supervision: Walking Alongside AuD Students, presented by Jackie Clark, PhD.
Learning Outcomes
After this course, learners will be able to:
- Identify and list the basic concepts around Experiential Learning.
- List the traits of high emotional intelligence and leadership.
- Explain how supervision differs from preceptorship.
Circle of Supervision
Through the years, I have served as a course instructor and clinical preceptor both on and off-campus. Having multiple roles has allowed me to work with students on many levels. To begin, I wanted to give a brief overview of the phases of supervision before we dive deeper into the course. One type of supervision is educational. When we think about formal classroom interactions, those are considered more of a didactic educational exchange. Formal classroom interactions with students tend to be very methodical and organized. As we begin the journey with our students, we can have informal opportunities (i.e., questions after class, hallway discussions, office appointments) as well. Once trust is earned, non-academic exchanges will grow organically. When we think about non-academic exchanges, that is when great opportunities arise. It would be a shame for us to ignore those opportunities that we have. I am quite happy when students feel comfortable enough to discuss non-academic topics with me. It is a positive aspect for us to interact with our students in various and vibrant ways. It all goes back to an open-door policy. At UT Dallas, that is one of our mottoes, almost all of our faculty has an open door. Of course, my door's closed when I leave for the day, but it is an enriching way for us to be able to reach out. Clinical exchanges are another way we can start engaging in with our students.
Circle of Supervision
- Formal Didactic Academic Exchanges
- Informal Academic Exchanges
- Informal Non-Academic Exchanges
- Clinical Exchanges
- Between Patient Exchanges
- Outreach Programs
Endgame for Students
Traditionally, the definition of “endgame” is the stage of a chess game after a significant reduction of forces, and there are only a few last moves to make. The same occurs with our students. After we have finished polishing and molding in the academic and professional realm, we need to think about the endgame. The endgame is all-encompassing, and it becomes very organic. I have had students that become anxious and panicked, and I have to help them refocus. Often, that leads us down the pathway of holistic patient-centered care.
Different Roles When Working with Students
In the realm of supervision, there are several roles. The choices are whether we want to enter into clinical supervision as a mentor or preceptor. Ultimately, you will choose. Does it mean you are going to choose one role? Next, how do we define these roles?
Clinical Supervisor
A clinical supervisor has multiple facets. Classically, a clinical supervisor requires more of a face to face communication and gives clear direction, sometimes obtained through observation. Daily evaluation is a responsibility clinical supervisors hold. Of course, there are hybrids and variations that are within this role. A clinical supervisor can be complementary to other forms of supervision as well (i.e., performance monitoring, observing actions and behaviors, assist with monitoring). We want to help the learner focus on behaviors as well as consequences. Often, you will see that the supervisor is associated with a job. With audiology, we tend to merge the term supervisor with preceptor and mentor.
Mentor
Often, we see a mentor as a voluntary relationship, where you have a mentee who identifies and links with a chosen mentor. The mentor is an encourager for the mentee or learner. For this to be successful, the role of a mentor is offering non-judgmental listening. Mentorship will aid the learner in integrating themselves among other peers. This could be within the profession, or it could also be within an institution or both. We have a lot of undefined outcomes when we have a mentor-mentee relationship. This relationship is not built upon performance monitoring. Instead, a mentorship is a beautiful way to improve confidence building. As a mentor, you know you have succeeded when the mentee understands that you are maintaining confidentiality. Only then are they able to grow and flourish under that particular role with you as the mentor.
Qualities of a mentor:
- Voluntary Relationship -- typically mentee chooses a mentor
- Encourager
- Offer Non-Judgmental Listening
- Help with Continued Socialization within Profession/Institution
- Undefined Outcomes
- Confidence Building
- Maintains Confidentiality
Strategies of a mentor. As I mentioned earlier, mentorship does not involve performance evaluation and can be a very formal or informal process. Sometimes it is looking back over a period of time with the mentee to see their progress. Again, the important thing is, we are not looking to be responsible for the day to day activities or solving problems. As a mentor, we are not evaluating an individual's progress or teaching specific position related skills or tasks. Mentoring is all-encompassing and is an excellent organic way to help them move forward and become socialized within that institution. When you enter into a mentorship, you have to consider the expectation or length of mentoring. A formal mentoring relationship may last 6 to 12 months long. It is enriching for both parties when we think about the opportunities that are there as a mentor. Those are some great opportunities for us to grow as well as help our profession grow.
Preceptor
The preceptor is appointed, and the learner does not typically choose them. A preceptor is someone who is an experienced practitioner. They are providing oversight during clinical practice, and some of it might be supervision as far as an employee and direct line of report. The preceptor is going to be individualized to the mentee. The preceptor will facilitate applying theory to practice. The preceptor is also very critical in assisting the students and learner by applying the knowledge that is gained through a didactic program. I frequently think of it as you're adding more of the finishing polish. Sometimes there are a few rough edges that we need to polish off a little bit more.
What makes an effective preceptor? Communication is important. A successful preceptor would have a broad knowledge base and be open to conflicting ideas and opinions. They would need the capability of expressing goals and expectations. I often say that as a profession, we are communicatively disordered because we tend not to express things clearly. Sometimes it doesn't hurt to be direct with our communication to ensure we are clear. When a question comes up, we should not feel attacked, but instead, remain open. Ultimately, what is critical is connecting that information to broader concepts. That will allow us to capture and maintain the attention of the learner.
We need to assess where the learner is at. What are their knowledge, attitudes, and skills? We want to provide opportunities for the learner, not only to tell us what is going on but for them to reflect. An example to facilitate reflection is, "tell me from today's appointment, what are you most proud of?" "Looking back, do you wish you'd done differently?" This open communication allows us to be more constructive and give useful feedback.
We also want to look at practice and teaching skills. An effective role model can demonstrate skillful interactions with patients and colleagues or staff by presenting information with clarity. You also want to make sure that when you are conveying the skill, it generates some interest in the subject matter. Sometimes we have to understand we don't need to be repetitive. There is a balance between clinical and teaching responsibilities.
We want to motivate the learner. If the learner is having difficulty, it is essential to engage them in conversation. By promoting active involvement from the leaner, we can translate some of the specifics in the principles and theory. As preceptors, we have an opportunity of demonstrating enjoyment, enthusiasm, and a passion for patient care. Ultimately, the questions that we might ask is, "So what do you think is going on?" Then consider the multiple interpretations of the data we are seeing. It is an excellent way for us to tap into that learner's thought process and knowledge.
Clinical teaching strategies of a preceptor.
- Modeling/demonstrating
- Observation
- Case Presentation
- Direct Questioning
- Think Aloud Method
- Coaching
Modeling is an excellent way for a preceptor to demonstrate clinical skills and reasoning. This strategy is useful, especially with new students, even with advanced concepts, it is still valuable for the advanced learner. Having the preceptor and student observe each other is another excellent strategy by stepping back and allowing the learner to engage with the patient while being prepared to jump in as needed. If it's not a huge error, let the student continue to work their way through, and that's a hard thing for us to do. Case presentation is another great way for us to tap into the student's ability to identify salient information about the case. Direct questioning, of course, is also essential. Ultimately, when we do direct questioning, we want to be very cautious that we don't put the student on an uncomfortable spot. If you start seeing that they are nervous, try to throw lifelines so that we can work our way through it without causing a lot of undue duress. We don't want to question the learner's actions in front of others. I will also think aloud but encourage the student to tell me what they are thinking. We want to be non-confrontational. Lastly, coaching by providing verbal cues and positive reinforcement can go a long way. Which role do you want to have in your student's journey? A clinical supervisor, mentor, or preceptor?
Experiential Learning
There's a variety of ways that we can enhance learning for the student. Experiential learning (i.e., experiential education), is looking at the process of learning. You're using reflection as part of this process, and there's a greater emphasis on individual learning. An example of Experiential Learning is asking, "What are we doing? Why are we doing it? What does this help you do that's important?" There are more concrete issues related to the learner and the learning context. Hands-on learning is one great form of experiential learning. In our profession, we have some great technology, so that gives us that hands-on learning. Experiential Learning can take place outside of the classroom. This can be in the form of clinical experiences and practicums. However, to gain knowledge, the learner must have four abilities.
- Willing to actively be involved and invested in the experience.
- Have the capacity to reflect on that experience.
- Posses and use their analytical skills so that they can conceptualize the experience.
- Possess decision making and problem-solving skills.
An apprenticeship provides an opportunity to try out for a job, usually with an experienced professional in the field (e.g., found in Education). Fellowships are another great way with that experiential learning. Fellowships from educational institutions provide tuition or aid to support the training of students for a period of time. Clinical experiences will provide hands-on experiences with some duration of time for the study that we see in audiology or nursing. Then we also have some other interesting areas that are available, depending on the program. I'm very fortunate that I have a study abroad project that allows me to engage with students on other platforms. This gives the student and learner a way to engage in different cultures and environments. Study abroad, as experiential learning, can provide a student the opportunity to learn about culture as well as themselves.
How Do You Get to the Endgame?
Ultimately, we want to meet the learner where they are at. When we start thinking about an endgame, we have opportunities to play a part because of our experience as preceptors, mentors, and supervisors. I'm hopeful that as we conclude this talk that I might convince you to make leadership and interacting with our learners in different ways, your endgame. Audiologists have excellent technical skills, and along with the ever-changing technology, we have so much to offer these students. We are integrating information that we have obtained and determined a pathway of action. The other thing that we have learned are soft skills of conveying critical information, and the capability to empathically communicate our conclusions to all those that we serve.
Leadership
If we can influence the learner, that learner will eventually become our professional colleague. As clinicians, we have a responsibility of being the leaders for these learners and inspiring them to take on that gauntlet of leadership. We have the opportunity to provide the time for each learner to reflect and obtain a deep understanding of the way we do things. In hopes that this will lead them to be reflective of why they are doing certain things. In the end, we want to get to our endgame by empowering our future leaders while we are also leaders.
Qualities of a leader. Leaders accept responsibility for failures and do not throw anyone under the bus. They are accountable so that there's no blame. Leaders do not claim credit for the success of the team because the whole team is the success. Also, the quality that's most admired with leaders is being decisive. Imagine a very indecisive leader who continually changes directions; it's like a ship without a sail.
What makes a successful leader? First and foremost, a successful leader is going to lead with honesty and integrity. Those are the very authentic ones. We see those individuals that have real executive presence. A successful leader is always able to look at the big picture. Excellent leaders build relationships. They can build those relationships because they are approachable. I still like to say actions speak volumes. A leader will actively listen. They understand that there are going to be hard messages that are unavoidable yet necessary. A leader will have the confidence to make hard decisions and move on.
Common elements in the art of leading.
- Vision
- Creativity
- Service above Self
- Team/Trust Building
- Emotional intelligence
Emotional Intelligence (EI)
If I'm stepping forward as a leader, then I also need to facilitate the learner to grow emotionally as well. You'll see a lot of the buzzword with emotional intelligence. The brain is hardwired to give emotion an upper hand. If we think about technical competence, then we also have to be able to control our emotional intelligence.
Self-awareness. With emotional intelligence, we have to have self-awareness. Personal competence is the ability to understand and recognize your moods, emotions, and drives. This involves what you say, do, and act and how they will impact others. That's an essential thing when we think about the emotional self-awareness. For us to grow, we need to look at what we're doing and how we are perceived.
Motivation. This is the ability to inspire others to be engaged. It's looking outward. How can I engage and work with others, so they are willing to give their full effort?
Empathy. This is an ability that I believe can be learned. Some people are more empathic than others. Empathy is the ability to be able to listen and fully understand. It allows us to be comfortable and aware of what the needs of others are.
Social skills. We could also think of social skills as the competence of relationship management ability. It is how we can influence others. As well as be able to handle conflict and work well with others. So, how am I going to manage that conflict? Inspirational leadership is also very critical when we think about social skills. Coaching, mentoring, and teamwork are examples of social skills.
Self-regulation. This part of emotional intelligence goes back to personal competence or knowing how to manage your emotion. We have all been in that situation when you start feeling stressed, and the amygdala is engaged because the brain is hardwired to give emotion the upper hand. When you start feeling like this, you have to know when to pump the brakes. That means you're going to have disruptive impulses. Being flexible and comfortable with new ideas often helps with that. It is emotional self-control and feeling adaptable. Keeping a positive outlook is vital to self-regulation.
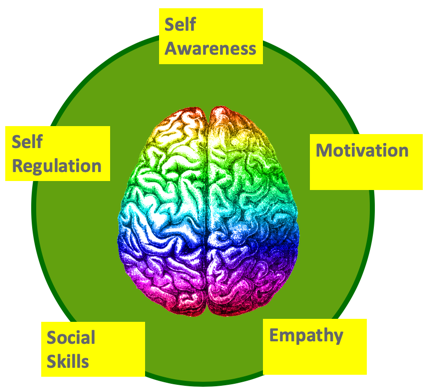
Figure 1. Emotional intelligence.
Daniel Goleman is one of the big gurus for emotional intelligence, and I would encourage you to look at some of the literature from Daniel Goleman. What do we mean by emotional intelligence? It is the capability to recognize your own emotions. You also need to identify the emotions of others. Discerning between different feelings and being able to label things appropriately is critical. We want to use that emotional information to guide our thinking and behavior. We want to make sure we keep our emotions in check. Managing our feelings will help us to adapt to environments.
Individuals with High EI
Individuals with high emotional intelligence have greater mental and physical health. These individuals keep their emotions intact during moments of stress, thus making them open and receptive to new ideas. It also leads to better job performance, as well as healthy self-esteem. It feeds into the leadership skills of having non-imposing views, the capability and capacity to listen and of course, maintaining enthusiasm. Those with high EI demonstrate a critical leadership skill of empathy. More recent studies have identified possible neural mechanisms of emotional intelligence. That's a fascinating realm of research that is being engaged in right now. I find that very exciting. Our brains are hard-wired to give our emotions an upper hand. We want to improve our technical skills so that our soft skills can improve. We need to control our emotional intelligence. My endgame has been to walk alongside each of the students. Sometimes the students won't allow that, so we have to be ready and open to students that might reject us. We also have to understand that they will become our professional colleagues once they graduate.
Conscious Leadership
Jim Dethmer has a book, The 15 Commitments of Conscious Leadership, where he comments on conscious leadership.
Cultivating self-awareness. Leaders become self-aware by monitoring and managing their strengths, motivations, and thoughts. I always say, lead with your strengths.
Check your influence. Who do you surround yourself with? When we start looking at an individual, we first look at the whole group. Are you happy with being the average sum of that group? Are you an outlier, or are you part of that group?
Inner strength. Tools like meditation, taking a walk, chanting, etc. can condition you to perform under stress so that you can avoid an emotional takeover. That's a great thing when we compare that conscious leadership to the unconscious leadership.
Unconscious Leadership
Those that demonstrate unconscious leadership are not true leaders. They usually rely on reactionary and non-strategic planning, where their ego runs the show. The mindset is very egocentric.
Conclusion
We also have to think about the words we use. Words are powerful when building relationships. They help us safeguard integrity and save face. I believe that if we all feel like we can be heard and respected, that's an important thing. Choosing our words wisely should be vital for us to remember as a preceptor, mentor, supervisor, or clinician. It's also worthwhile when we start looking at how we model and demonstrate to the learners. We can help the learner script what they want to say. We can role play with them on what they might want to say so that they have a much deeper understanding of the power of the words. Sir Isaac Newton said, "Tact is the art of making a point without making an enemy." "Diplomacy is the art of letting someone else have your way," by David Frost. We want to use a lot of tact and diplomacy. When we consider our learners, we can model by using role-play and scripting to help them understand tact and diplomacy.
I've shared with you my endgame, and I'm hopeful that I can convince each of you to make it your endgame. I hope that we can walk beside our students during these very formative years. We also have to recognize that we have an abundance of influence on future professional colleagues. Ultimately, we want them to be leaders of our profession because when we all retire, they will be the future of audiology.
References
Bariso, J. 11 Basic Practices of EI People. https://www.inc.com/justin-bariso/11-beneficial-habits-of-emotionally-intelligent-people.html. Retrieved 4-1-2019.
Biagoli, F., Chappelle, K.G. How to be an Efficient and Effective Preceptor. Family Practice Management, 17(3):18 (2010)
Eberly& Fong: Leading via the heart and mind: The roles of leader and follower emotions. The Leadership Quarterly, 24(5): pg696 – 711.
Goleman, D., Boyatzis, R.E., Mc Kee, A. Primal leadership: Realizing the power of emotional intelligence. Harvard Business School (2002).
Kolb, D. Experiential Learning: An experience as the source of learning and development. Englewood Cliffs, Prentice Hall. (1984)
Lazarus, J. Precepting101: Teaching strategies and tips for success for preceptors. Journal of Midwifery & Women’s Health, 61(s11-s21). (2016)
Mills, Francis, & Bonner. Mentoring, clinical supervision and preceptoring: Clarifying the conceptual definitions. Rural and Remote Health, 5(410). (online, 2005)
Steber, C, 8 Emotionally Intelligent persons have in common.https://www.bustle.com/p/8-habits-emotionally-intelligent-people-have-in-common-9326975. Retrieved 3-29-2019
Citation
Clark, J. (2019). Supervision: walking alongside AuD students. AudiologyOnline, Article 25580. Retrieved from https://www.audiologyonline.com

