
Editor’s Note: This text course is an edited transcript of an Oticon live webinar on AudiologyOnline. Download supplemental course materials.
Learning Objectives
Dr. Donald Schum: The learning objectives today are as follows: Participants will be able to list the typical reaction patterns that older adults will demonstrate when faced with physical and social limitations as they age; participants will be able to describe how changes in social interaction patterns may potentially make the person more at risk for accelerated cognitive decline; and finally, participants will be able to identify potential subtle changes in patient counseling to reflect what we know about social interaction patterns in older adults.
Age-Related Hearing Loss
As audiologists, it is important that we continue to learn about age-related hearing loss and the patients who are experiencing it, beyond the audiogram. I have become more interested in recent years of understanding older individuals within the context of the lives they lead to best understand how they want to use their hearing.
When we talk about speech understanding, in most contexts, we are referring to an interaction between humans: between the listener (in our case, a listener with a hearing impairment) and one or more talkers in a variety of different situations. When I talk about sociology and social situations, I am talking about it in a broad context. Any time the older adult comes in contact with another human being in the normal course of day-to-day living, those connections or interactions are affected by both the hearing impairment and also by other factors.
There are two photos shown in Figure 1. The woman on the left is in her garden, daydreaming, and the woman on the right is having a nice dinner with a male companion. Suppose that both women have the same degree of hearing loss. For which of these two individuals is hearing loss more relevant?

Figure 1. Two women with hearing loss in their daily lives.
The simple answer is that the woman on the right would have more of an issue because she is in a potentially difficult communication environment and trying to understand speech. But, what if the woman on the left would also like to be sitting in a restaurant having a nice conversation with a companion, but without even realizing it, has changed her social interaction patterns because of her hearing loss?
It is impossible to answer for whom the hearing loss is more relevant, because I gave you no information about their history. Just because the individual on the left is not using her hearing actively at this moment in time to understand speech, it does not mean that she does not want to be doing that.
Environment or Interaction?
There was an interesting project carried out 10 years ago by my Oticon colleagues from Eriksholm Research Center in Denmark. At that time, Oticon was very interested in the type of environments people find themselves in, or what we call auditory ecology. Søgaard Jensen and Nielsen (2005) used a classic dosimeter study where they sent a group of patients out with dosimeters to measure the characteristics of the acoustic environments in which they found themselves. They also had the patients fill out diaries about what they were doing at that point in time. They were checking to see whether or not patients were good reporters of their environments. They received the data back and they would look at the environments that the patients said they were in. For example, maybe the patient reported they were in the kitchen, then the car, and then at work. Then the researchers would look at the dosimeter and note the levels.
When they tried to bring together what patients were saying about hearing and the environments, they realized that there was not a correlation between the sound levels that they were seeing on the dosimeters and the troubles that the patients were reporting. The initial reaction was that the patients were poor reporters. To that end, they brought in a psychologist to conduct interviews. The researchers did not believe that they patients were lying, but they wanted to better understand their responses. The psychologist determined that when you ask a patient about having trouble listening, they do not talk about the environment specifically; they talk about an interaction that they had within an environment.
In other words, the sound level in the kitchen or the car or at work only matters it they are trying to use their hearing. If they are in a specific environment and are not using their hearing, then the acoustics of the environment do not matter. They only report problems when they try to use their hearing to interact with other people.
This was an interesting wake-up call to these researchers and to us as audiologists; we often only look at the acoustics of the environment. There is a program in your hearing aid for restaurants, car, music, et cetera. We do not necessarily look at it from an interaction standpoint.
Reactions to Body Change
It is important for us to recognize that we are not the only health care profession that deals with age-related body change. Age-related body change happens in many domains, and there are many other professional groups who are involved in the lives of older individuals as they are going through body change. I have several books on my bookshelf that talk about how aging is studied from many different perspectives, especially the physical, emotional, and social changes people go through as they get older. This presentation will look at these other fields and identify what lessons we can learn and perhaps apply to the audiological issue of treating patients with age-related hearing changes.
Denial
One of the classic reactions to age-related body change, including hearing loss, is denial. All audiologists know this, so many of us think that every patient who walks in the door is in denial. Let's make clear a few things about denial.
The first is that not every patient is in denial. There are many patients who come to us in a very good mental and emotional state about their hearing loss and are ready to do something effective. The second thing is something I learned when we hired a disability specialist to speak to a group of our customers. We asked this specialist to teach us how to get people out of denial. He reminded us that denial is a defense mechanism. It is a reaction that a person takes, usually involuntarily, when they are not emotionally ready to deal with a challenge to their well-being and psyche. It is natural and to be expected. Importantly though, he pointed out that it is usually just a stage. It is something that the person retreats to when they are dealing with a difficult circumstance, and then they will move through it.
His point to us was to expect and prepare for denial, but not look down on the patient because of denial. Understand that the best thing you can do is not try to get a person out of denial. Instead, help the patient move through denial. It is a matter of assisting the patient to deal with their emotional challenges. If you want to help improve their life by improving their hearing, you have to understand what denial is all about and help them move through it. I will talk a little bit more about techniques later in this talk.
Normalization and Passive Acceptance
Another important reaction pattern that many older adults will show when faced with age-related body change is normalization and passive acceptance. Normalization and passive acceptance is best summed up by the phrase, “This is just what happens when you get older.” In other words, there are many older adults who do not deny that something has changed. They do not deny that they should do something about it, but rather, they do not take action because they just expect things like this to happen as they age. They know when they get old, their bodies will fail, their eye sight will fail, their hearing will worsen, et cetera. They passively accept these changes and move on.
This common reaction pattern by older individuals is equally as difficult to audiologists to deal with. When a person is in denial, there are in conflict between what they know they should do and the fact that they are not ready to do it. With normalization and passive acceptance, there is no conflict. The person owns it. The problem, however, is when the person does not have any passion about what they are missing. In that case it is hard to motivate them to take action if they do not feel they are missing anything. They have resigned themselves to the fact that they are not going to have conversations or be as socially active as they used to be. We know as audiologists that is untrue, but that does not mean that the patient knows that. Dealing with someone who is in normalization and passive acceptance can be just as challenging as dealing with someone who is going through denial.
When you think about normalization and passive acceptance, let’s remember where that can come from. Hearing loss typically does not happen overnight in most adults. Like many other health issues, it is gradual. Some people have the attitude that they want to grow old gracefully and not fight every little thing that is changing about them. “If I went to the doctor every time something ached in my body, I would be at the doctor all the time,” is a common theme heard from our patients. Those are reasonable responses, but it works against the idea of someone doing something positive about their hearing loss.
Since their bodies are always changing, many older individuals have a hard time knowing if they need to talk to a professional about what they are facing. Many of you know the problems that we run into with primary care physicians, who, if the person does not have a life-threatening disease, may say that because the person is not dying that they will be okay. However, we cannot always lay this on the doorstep of the primary care physician. It has to come back to the patient and us trying to motivate the patient to want to do something about their hearing. If they do not know if they need to talk to a professional, you may never see them, and that is part of the problem.
Self-Image
The other factor to remember is that there are self-image challenges that patients can run into as they age. They know they are not as young as used to be. They cannot do all the things they used to do. When it comes to health care issues, the psychology in the area of aging will point out that symptom minimization, or telling yourself it is not so bad, does have a positive effect, because it helps to protect your self-image.
Sometimes when people discount or minimize their health issues, it is because they are trying to protect their self-image. It is a form of denial, in a sense, because they do not want to say out loud that they are not as young as they used to be. There are a lot of reasons why people will not make a big deal about their hearing loss, and it has nothing to do with their hearing. It has everything to do with their psyche and the idea of getting older.
Another thing to remember is to remind ourselves of is where hearing falls in the progression of aging. When someone in their late 60's shows up in your clinic and this is the first time they have talked to someone about their hearing, it is important to remember that this is not the first time they have been to see a health care professional about something that has changed in their body. Of all the things in the human body that change as a person gets older, hearing is late on the list.
Because of that, by the time a person recognizes they have a hearing loss is, they may have already become an expert in dealing with their own body change. I am not saying they deal with hearing loss the same way they would deal with diabetes, for example, but there is some commonality to the way they react. Some people will be the type to have every ailment fixed; others may be passive acceptors where they are “not fixing that too.” If hearing loss falls into the category of things they do not worry about, it may not be that they are avoiding treatment for their hearing loss, but rather that they are tired of dealing with “stuff” in general. This does not mean we should not try, but we have to recognize where those feelings might be coming from and factor that into our counseling approach.
Confidence and Self-Efficacy
Another theme that psychologists talk about when it comes to aging is confidence and self-efficacy. There are a lot of positive health benefits to an older individual maintaining a positive sense that they are still vital, competent, and that they can still do things. If you are in your 20’s or 30’s, you think you are on the top of the world and will always be. However, stop and think about the way our Western society treats older individuals. There are many subtleties that occur as an individual ages that perpetuate a message that they are not as valued or vital anymore. It is not because people are doing that consciously as a way to be mean or unloving; it is just the way our society works. When you look at the following list, you can understand where there might be a sense of erosion or self-confidence and self-efficacy.
- Children grow up, start own families and no longer use parents as a safety net
- Replaced at work by a younger person
- No longer in work force holding a position of responsibility
- Physical limits on the activities that can be enjoyed
- Falling behind in technology uptake
- Out of touch with popular culture
- Friends pass away or move away
- Need care assistance
- Restricted from activities, such as driving
One of the things that would be pointed out by the sociologist or psychologist is that a person needs to have a sense that they can achieve and be successful when they take on a new challenge. Doing something about their hearing is taking on a new challenge. Patients need to have the sense that if they decide to become a hearing aid user, that they will jump in with both feet and make it work.
As each of you know, hearing aids are not a perfect solution for sensorineural hearing loss. That is the nature of the condition that we treat. We provide an incomplete solution to the problem. The patient’s willingness to accept an incomplete solution and correct for communication environments is something that requires confidence.
There is something called the SOC model of reaction to aging. This stands for selectivity, optimization, and compensation. This is the reaction pattern that older individuals could show when they are faced with age-related body change.
Selectivity
Selectivity means that as a person ages and something has changed about their body that they will select which activities that they choose to do based on their new level of capability. If they cannot participate in a particular type of event or activity that they used to because something has changed about their body, then they will choose to spend their time doing other things. Maybe they used to be more social and go to more parties. Now they spend more time reading and watching TV.
Optimization
Optimization is when a person tries to get the most out of their limited skills. These are the types who might believe that they have to learn to lip read or just listen harder. They are willing to work harder to get better at the thing that is not as good as it used to be. For example, if you are an aging golfer and cannot drive the ball as far and become much more dependent on your short game, then you may start to focus on perfecting your short game. They can make up for the fact that they have lost distance by being much more accurate in the short game.
Compensation
Compensation means that you are willing to take technical assistance to make up for something that you cannot do anymore, such as using a walker or a cane, using eyeglasses, or using amplification. This means that you are willing to admit to the fact that you need some sort of technical intervention in order to do the things that you used to do. Selectivity is by far the most common reaction pattern in older adults. They stop doing what they do not do well anymore and spend more time doing the things that they can still do well.
Compensation is the least common reaction pattern. We do not want people to remove themselves from social situations. We do not want people to decide that they cannot count on their hearing so they do not use their hearing as much. We want people to continue to have motivation to hear well, and we want to help them out because we know how important it is. The problem is that the likelihood of people using amplification when they really need it is well below 50%. This may very well have something to do with a general type of reaction pattern that older adults show when they are faced with age-related body change.
Effort
Communicating takes effort, and communicating with hearing loss takes more effort. Effort, or the willingness to try, is something that the patient can dial up or down. A former colleague of mine, Therese Thorstholm who is an anthropologist, worked for Oticon in our central office in Copenhagen. Anthropology is the study of individuals within groups and humans.
Therese did her Master’s thesis by embedding herself in a social organization in one of the neighborhoods in the Copenhagen area where they have social clubs for older retired individuals. Once a week, the people get together for an afternoon and spend time together socializing. I know that some care facilities in the United States that will do this, but in Denmark, these are just people who live in the neighborhood and get together. This is a prevalent Danish custom. She observed how the people used their hearing and communication skills within the social context. It was an interesting project.
The difference between audiology and anthropology is that audiology is a clinical discipline. We want to do something to help people overcome a health problem. We are interventionalistic by nature. We are fixers. The job of an anthropologist is to be observational. An anthropologist wants to observe, record, and analyze, but not effect. As audiologists, we want to fix things, whereas anthropologists want to understand how things are. It is a different type of discipline.
One of the gentleman in Therese’s group made a point about the effort of communication. There is a distinction between having to direct my attention to what is being said and that someone is merely saying something. In other words, when your hearing is not so good and you know it takes effort, then you can decide whether or not you are going to work hard to be a listener. That decision to work hard is going to be driven by motivation. Is it valuable enough for you to work hard to understand better?
Therese told me another story that I think is interesting. She was interviewing a couple; a man with hearing loss who wore hearing aids, and his wife. The wife was commenting that he seemed to do so much better with his hearing when they were at noisy busy social clubs once a week than when they were home alone together in their quiet apartment. She was very frustrated that she would try to communicate with him and he did not seem to be able to hear her, but when they would go to these loud places, he would seem to do fine.
Therese interviewed the husband to try to determine what was happening. He told her that when he is in those social clubs, he really wants to be there and enjoys the people. He is willing to work at being a listener because it is so valuable. Being at home is his down time. That is when he does not want to have to work so hard as a listener. If the wife is communicating with him from room to room and he cannot see her face, he is not willing to try very hard because that is when he wants to relax. Hearing loss requires more effort. That is the nature of the condition that we treat. We have to understand that a person can actively decide whether or not they are going to turn effort up or down at any moment in time.
Communication as a Health Issue
There is concern about doing everything we possibly can for older adults to try to maintain good health, as if aging is a threat to health. Communication is a big part of the health issue and goes beyond audiology. Active aging is a positive concept, centered on the ability to continue to participate in activities and live a vibrant life. The three pillars of active aging are participation, health, and security (Kalache, Barreto & Keller, 2005).
Successful Aging
Participation, which is the ability to interact with other individuals, is a big part of a general desire for older individuals to be as successful, happy, and healthy as possible. There is a concept called successful aging. Many of you know older individuals who seem to be handling aging very well with a positive attitude. They seem to be very fortunate about their health and are very active in the things that they do. You may know of other individuals where aging hit them abruptly and they do not seem to be able to participate and do the things that they want to do. The point is that there are determinants to what constitutes successful aging.
Based on that idea, there are three determinants of what constitutes successful aging: being free from disease, maintaining good cognitive function, and maintaining quality contacts with people and activities. These ideas come from the general field of aging and psychology. There is not a lot that we can do about being free from disease and maintaining good cognitive function, but we can participate in maintaining quality contacts with people and activities. Part of successful aging is still participating in the things you have always done. Remember one of the classic reaction patterns when people get older is selectivity, meaning that they will select only those activities that they seem to be successful at and avoid the ones that challenge them.
Cognitive Decline
Part of the concern of lack of socialization is related to cognitive decline. Aside from our concern about whether or not people can do the things that they have always wanted to do, there is a real health concern going on, including Alzheimer’s and cognitive decline. Duke University published an overview article looking at the published causes of Alzheimer’s and cognitive decline and the things that seem to prevent Alzheimer’s and cognitive decline (Williams, Plassman, Burke, Holsinger, & Benjamin, 2010). They came up with a list of the greatest threats and predictors of Alzheimer’s and cognitive decline, and then they listed things that they thought would protect people from cognitive decline. These are listed below.
Greatest Risk Factors:
- Diabetes
- Genetic predisposition
- Smoking
- Depression
Protective Factors:
- Cognitive Engagement
- Physical Activity
Of the protective factors, there is physical activity, which means that if a person is physically healthy and active, it helps with blood flow and physiologic functions. Cognitive engagement is the other factor. Cognitive engagement is the strongest predictor of a person being able to avoid early cognitive decline. It is a use-it-or-lose it situation. There is solid evidence suggesting that strong cognitive activity can protect the brain to some degree from early cognitive decline. A large part of social engagement is cognitive engagement. It is not a passive action. There is a lot of push to keep older individuals socially active in order to prevent cognitive decline.
Relationships: Quality and Quantity
If speech communication is an interaction between humans, then we have to understand the typical relationship patterns among older adults. One of the observations that comes out of the field of sociology of aging is that the number of relationships that a person has changes as they get older; there is a clear decline in the number of relationships that a person can maintain. Obviously, some of this is related to vocational issues when a person retires. Their circle of interaction becomes smaller, but there are other things like family changes. Interestingly, while the number of relationships decline, the depth of relationships increase as a person gets older.
Oftentimes, we tend to focus on the numbers. Are you not in as many social situations as you used to be? Do you not spend as much time with your friends? What the people in the sociology of aging point out is that you should expect people not to interact with as many people when they get older. However, you want to focus on making sure that the individuals are maintaining meaningful, deep relationships with the people that they are still in contact with. To me, that is one of the best lessons I think that you can take away from this talk. Recognize that depth is going to be more important than numbers. It is a quality issue, not a quantity issue.
Framilies
In relation to this, let’s talk about framilies, or friends and families. They are not the same. As an audiologist, how often you have said “friends and families” to a patient? “Do you still want to maintain contact with your friends and family? Do you have problems hearing your friends and family?” We group them together, almost as a single entity. The people in the psychology and sociology of aging point out that the relationships of friends and families are not always the same. Adult friendships are a good sign of successful aging because it takes effort to maintain friendships as you get older.
There are too many limitations that occur in an older adults’ life where maintaining friendships becomes harder. There are physical limitations to moving around. There are practical limitations, especially when a person retires. If many of their friendships were based on their work environment, then that would be a threat to some of their best friendships. Maintaining adult friendships is a very good predictor of overall psychological well-being for older adults. It means they are willing to put the effort into maintaining a friendship.
Think more deeply about your counseling when trying to motivate an older adult who is on the fence about getting amplification. Do not discount the differences between friends and family. Sometimes family relationships are also very positive and important to individuals. However, you do not get to pick your family. If, for example, the grown children of an older adult who is having hearing problems are part of the picture, the grown children will still communicate with their mother or father. They may struggle more and be more frustrated by it, but they are still going to maintain that relationship because they are family. Friendships are voluntary. If they are willing to put the effort into maintaining the friendship, then they probably value that friendship highly, and that can be a good handle for you to use to help motivate the person to do something positive about their hearing.
Loneliness
Loneliness is another prominent factor that psychologists are concerned about. It is a solid predictor of declining health. If a person gets lonely, they start to get depressed and they do not take care of themselves. Other health issues start to arise, and then they get more depressed. It is a vicious downward cycle. One of the observations made about the health risk of loneliness is that it tends to be related to the depth of relationships, not the number of relationships. In other words, you can have a lot of friends but still be lonely.
It is a concern that older adults, especially those who lose a spouse or become physically disconnected with their family, lack of depth of relationships. From a counseling standpoint, we need to keep the focus on good relationships, whether it is to family or friends. Talk about how deep those relationships are, not how many they have. If there is only one person that is important for an older person to interact with, then that is enough, as long as you can get the person to talk about the depth of that relationship and realize that the hearing loss might be compromising the depth of that relationship.
Ear Miles Project
Another project out of our Eriksholm Research Group was an overview project to look at which factors predict help-seeking for patients with hearing loss. In other words, what aspects of a person’s complete life can predict whether or not a person would seek out help for their hearing, get hearing aids, and be successful in using hearing aids? They looked at published studies in our field and came back with some interesting observations.
The following items are the common factors that have been talked about as being predictors of motivation in patients.
- Age
- Gender
- Measured Hearing Loss
- Duration of Loss
- Socioeconomic Status
- Health
- Expectations
- Activity Level
The conclusion of the Eriksholm researchers in this project was that none of these were consistently related to help-seeking, obtaining hearing aids, or the benefit they could receive from hearing aids.
One predictive factor that made sense was self-perceived hearing difficulties. The patient has to feel that hearing is standing in their way. This speaks directly to the problem-based counseling that we should be doing with patients. It does not matter what the audiogram says. You are not in this to convince a person that they have threshold change; you are in it to discuss the problems and how they feel about those problems. Then, if you connect that with depth of relationships in friendships and family and the likelihood of the person showing passive acceptance and normalization, it brings the counseling to a different place. Some audiologists are good at this already, but I also understand the tendency in our field to talk numbers and levels, as that is our comfort level. There is much to learn from other disciplines about age-related body changes and viewing it from the patient’s perspective.
Patient-centered is almost becoming a throw-away term in our field, like evidence-based practice. It is an easy thing to say, but a harder thing to live. Patient-centered means that you have to understand all aspects that are relevant about the patient. Viewing hearing loss from a sociological standpoint of how people want to use their hearing and how they want to interact is a good lesson for us.
Internet Surveys
We did an internet-based survey as a means to come up with new questions to go into our fitting software. The following question is one that did not end up in the software because it did not tell us anything about how to change the effect of the hearing aid. However, I thought the results of this question were very interesting. The question was:
When at a social gathering, I would prefer to:
____ Have a quiet conversation with one person
____ Participate in a group discussion
This was done with 92 first-time hearing aid users with the average age of 73. Think about how you would answer this question. This, in fact, has nothing to do with a hearing loss. Some people would rather have a quiet conversation with one person at a time, and others like to be part of group discussion. The answers to this survey question were split nearly 50/50, and it was not related to age or the audiogram. People inherently have different social personalities. We need to remember that communication is not always related to hearing, and it is not always related to aging. Sometimes it is related to who the person is.
Another survey last year included 421 non-users of amplification with an age range of 55 to 75. It was a large study, and I was trying to pin down socialization issues related with aging Baby Boomers. It was based on much of the literature in this area and asked the participants to agree or disagree to the statements. One of the items on this survey said, “Over the past several years, I do not seem to be in as many social situations as I used to.” In this age group when hearing loss is becoming relevant for people, I was looking to see if there was a relationship. The distribution of answers are shown in Figure 2.
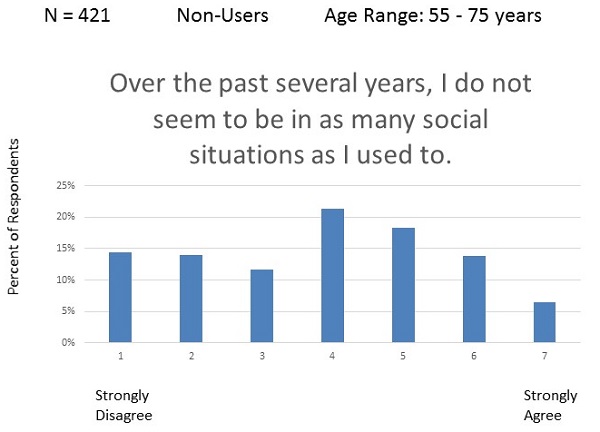
Figure 2. Distribution of answers to survey item related to social situations.
You can see that the answers are split across the board. Rarely do you see data that does not show a strong point somewhere in the middle. Interestingly, there were no simple age or hearing loss correlations. We asked the people to rate their hearing, and with 421 people, we had to base “hearing loss” it on their rated hearing abilities. The problem was that they all thought they were doing well with their hearing. We did have an age distribution, and it was not directly related to how old they were or what they thought about their hearing. This goes back to the idea that people are people; there are just some people who are going to be more active and others who are not.
We did not want to stop there because we thought there might be more to this question. With over 30 questions in the survey and over 420 participants, we collected a lot of data. We submitted the project to factor analysis, and the following list shows the common themes that we observed in the way the people responded:
- Willingness to take action
- Retirement viewed as “gearing down”
- Sociability
- Self-efficacy
- Acceptance of aging
Willingness to Take Action
When we used the factor analysis, we did see that the answers to this question were predicted by three of the factors. One of them was the willingness to take action in a negative way. In Figure 2, the left side of the scale means you are more social, and the right side of the scale means you are less social. People on the right side of the scale were not very willing to do anything about their hearing loss. That is the passive acceptance. As you get older, you just cannot expect to do as you used to.
Acceptance of Aging
Acceptance of aging, which is a little bit different, also relates. Those who rated themselves as a 5, 6, or 7 are more likely to say, “You are just going to get old. You have to accept it.” People on the other end of the scale, however, would say, “You might be getting older, but that does not mean your life has to change.” That makes sense.
Gearing Down in Retirement
The third factor was that retirement was viewed as a time to gear down. These are people who see their retirement years as a time to slow down and do less. Those are the people who felt less social. People who saw retirement as the opportunity to do the things they have been putting off are the ones who say that they are more social than they have ever been. One of the things this said to me is that this is not directly related to hearing, but more to who that person is.
The Health Belief Model by George (2001) is a list of concepts that will drive a person to do something about their hearing loss. These include susceptibility, symptom severity, perceived or expected benefits, perceived or expected costs, and self-efficacy. We see a recurring theme of how important it is for people to feel like they can do things well.
Counseling Approaches
Motivational Interviewing
Motivational interviewing is a good counseling strategy that makes a lot of sense in our field. Motivational interviewing is based on the concept that a patient has to make a decision to change. It was designed to help the person get to a point where they can make a good positive change in their life. If you are looking for a different way to gear up your counseling approach, read more about motivational interviewing at www.motivationalinterview.org.
Hearing Loss as a Disruptor of Socialization
When you talk to patients, try viewing hearing loss as a disruptor of socialization and not just communication. In other words, it is not just that they have trouble hearing and understanding speech, but rather is their hearing loss getting in the way of doing what they want to be doing? That speaks more to motivating them and to see the loss as something more than they may be willing to admit.
Moving from how they feel about their hearing loss to what they miss because of the hearing loss comes from motivational interviewing. This comes out of the denial issue that if they are not doing something about the hearing loss because it is a reflection that they are getting older and they are not ready to deal with it, that you have to accept that and acknowledge that they are going to be in that place. Then you have to work to move them through that denial stage. Motivational interviewing is good at giving suggestions in how to help people move through the denial stage. One of those things is what do they miss because of the hearing loss. What is the cost of not taking action?
The third factor, especially with Baby Boomers, is the idea of a second life. Once they retire, they can go and do the things they have always wanted to do. That can be a solid motivational factor for them to get them to do something about their hearing loss in order to be able to participate the way they have always wanted to.
Take Home: Focus on the “Who”
The best message I can impart with you is to focus on the “who.” Do not focus on “where” or “how often.” That is the way we as audiologists generally approach the discussion with patients - we ask about where they do not hear well or how often they are in those situations. From a socialization standpoint, instead focus on the “who.” With whom are they having trouble communicating? How valuable is it for them to maintain good communication with those people?
Focus on the depth of the relationships, especially if you can get patients to talk about their friendships. Focus on what they are missing by not being able to communicate well with the people who are the most important to them. Socialization is very important, and it varies from person to person, but it can be a very strong motivational factor to get a person to want to do something positive about their hearing loss.
References
George, L. (2001). The social psychology of health. In R. Binstock & L. George (Eds.), Handbook of aging and the social sciences (pp. 217-237). New York, NY: Academic Press.
Kalache, A., Barreto, S. M., & Keller, I. (2005). Global ageing: The demographic revolution in all cultures and societies. In M. L. Johnson (Ed.), The Cambridge Handbook of Age and Ageing (30-47). Cambridge: Cambridge University Press.
Søgaard Jensen, N., & Nielsen, C. (2005). Auditory ecology in a group of experienced hearing-aid users: Can knowledge about hearing-aid users' auditory ecology improve their rehabilitation? Proceedings of the 22ndDanavox Symposium.
Williams, J. W., Plassman, B. L., Burke, J., Holsinger, T., & Benjamin, S. (2010). Preventing Alzheimer’s disease and cognitive decline. Evidence Reports/Technology Assessments, No. 193. Rockville, MD: Agency for Healthcare Research and Quality. Available from: https://www.ncbi.nlm.nih.gov/books/NBK47456/
Cite this Content as:
Schum, D. (2015, July). The Sociology of age-related hearing loss. AudiologyOnline, Article 14504. Retrieved from https://www.audiologyonline.com.

