Learning Objectives
After this course, participants will be able to:
- List the types of individuals who are particularly affected by temporal cues.
- List the advantages of using fast-acting and slow acting compression.
- List the considerations behind a variable speed compressor.
Introduction
The concept of compression hasn't changed much in the last many years, but the focus on understanding compression has shifted in a significant way. If we understand the different parameters involved in the compressor, we will be better able to choose the right technology for our patients.
Understanding Compression
We can look at compression from three different aspects, similar to how we look at sound. When we talk about sound, there is the frequency aspect, the intensity aspect, and also the time aspect. We can think about compression in this same manner with these same three parameters.
The frequency aspect relates to the number of channels in the compression; the bandwidth of the system. Intensity refers to which gain parameter we adjust; the gain parameter of the soft sounds, loud sounds, and so forth. The time aspect of compression refers to the time constants, or the attack and release time of the system. All three of these parameters interact to result in the final signal that the patient would hear.
In the last several years, we have been more focused on the frequency and intensity domains of compression. Back 20 years ago, when we started talking about compression, the focus was on how to determine the compression ratio. How do we do loudness scaling so that we give patients the perfect compression ratio on the hearing aid?
In Figure 1, we can see that someone with normal hearing would start rating a sound at 30 dB to be very soft, and as the intensity increases, the person rates that sound to be louder.
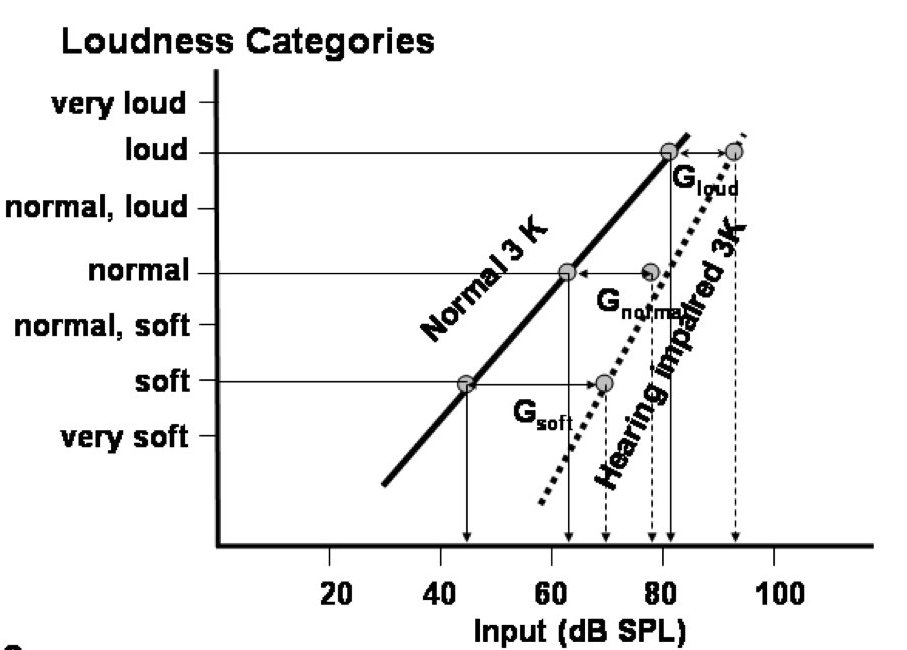
Figure 1. Determining compression ratio, normal hearing.
By the same token, a hearing-impaired person would perhaps need a sound to be 65 dB to be very soft, and it increases as the intensity increases. The difference is the gain level. The difference in the input level between the hearing-impaired and the normal hearing person to reach a particular sound level (such as soft, normal, or loud), is then taken to calculate the compression ratio (Figure 2). We can see that the loudness, the output level for the hearing-impaired person to reach a particular sound level is plotted against the loudness level or the intensity level for the normal hearing person to hear. When we plot the soft sound, normal sound, and loud sound, we can then calculate the compression ratio. In this case, we are talking about a static compression ratio of 1.8.
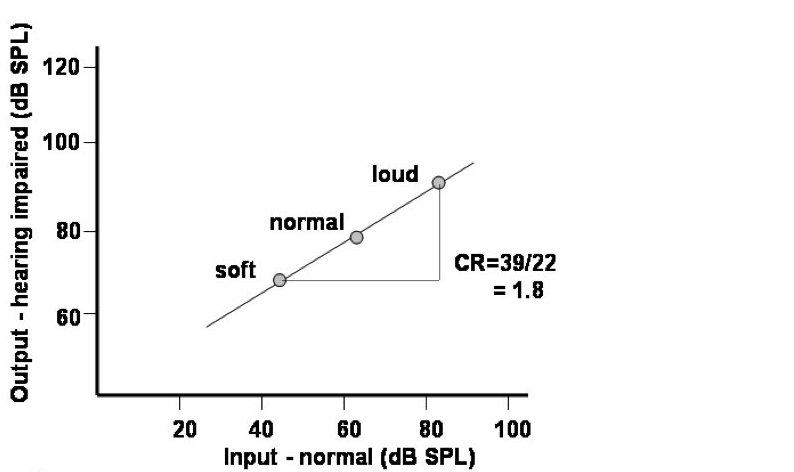
Figure 2. Determining compression ratio, hearing impaired.
Compression is Dynamic
These days, we understand that compression is not a static concept. In other words, when we say a hearing aid has a compression system, the compression ratio for that hearing aid is not a static number. Indeed, the compression ratio on a compression hearing aid can be affected by the number of channels within the system itself, how much venting the compression system is using, what the compression threshold is, as well as the time constants. All these factors can interact so that the compression ratio that the person uses in real life, or what we call the effective compression ratio, could be very different than what is reported on the specification sheet. It is important to understand that compression is a dynamic system, meaning that what the person experiences may not be what you see on the spec sheet.
The Temporal Waveform
In the last 10 to 15 years, more and more research has been conducted on the importance of temporal cues, and how they affect our speech understanding. If you look at the waveform on the top of Figure 3, you see a signal that has very well-defined peaks and valleys. The waveform at the bottom of Figure 3 is that same waveform compressed, and it does not show the same temporal pattern.
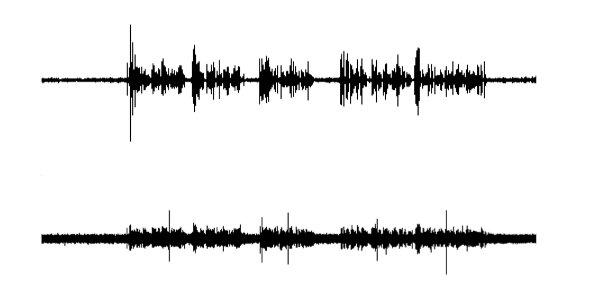
Figure 3. Importance of temporal nuances on cognition is shown in this waveform; the top image is the waveform uncompressed with defined peaks and valleys; the bottom image is the same waveform compressed, which does not show the same temporal pattern.
Populations Sensitive to the Temporal Waveform
Over the last two decades, we have found that there are some categories of patients who are especially sensitive to the temporal waveform. The first group includes people with low cognitive capacity, such as those with a poor working memory. Another category includes individuals who have a hard time understanding speech when there are few contextual cues in the conversation. If you cannot guess what you are hearing, then the temporal waveform becomes very important. By the same token, elderly individuals are especially dependent on the temporal waveform for extra information (which may be considered as under the same category as the low cognitive capacity). A fourth category of patients who are also especially dependent on the temporal waveform are people with more severe hearing loss. These people, possibly because of their poor hearing sensitivity, are not able to obtain spectral cues from the signal itself, so they're more reliant on temporal cues within the signal that can help them understand. These four categories of patients are more dependent on the envelope of the signal, as well as the fine structures within the temporal waveform (Figure 4).
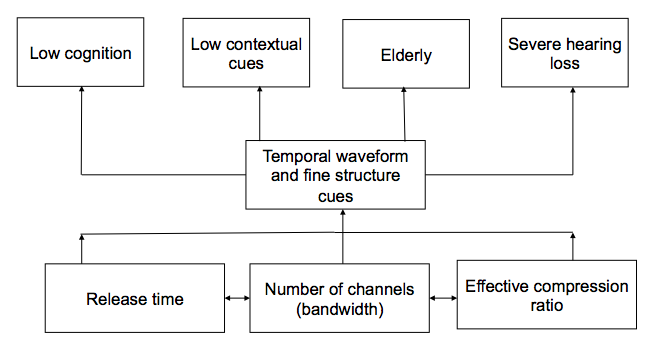
Figure 4. People sensitive to temporal waveform and fine structure cues.
Factors Affecting the Temporal Waveform
What are the factors that could affect the temporal waveform, the envelope, as well as the fine structure cues? One is the release time of the hearing aid; the speed of the release time can affect the temporal waveform of the signal. The second important thing to recognize is the number of channels within the hearing aid. In general, the greater number of channels, the more adverse effect it has on a temporal waveform. You smear the waveform more if there are more channels within the system itself, and we will talk more about that later. The third important aspect is the effective compression ratio, which is also affected by the venting in the hearing aid.
Effect of Release Time on Temporal Cues
In the last 20 years there has been a lot of research on the importance of the release time. One study was conducted in the mid-1990’s by Arlene Neuman and colleagues at City University of New York (1995; 1998). Their findings indicate that both normal hearing and hearing-impaired people prefer a longer release time. The longer release time, the higher the preference, the better the sound quality. These results were replicated in a study by Martin Hanson (2002), who was with Widex at that time. He found that the longer the release time, people liked the sound quality much better. These two studies demonstrated that whether you have normal hearing or hearing impairment, longer release time is much better for sound quality than a shorter release time.
In the last few years, there have been more studies demonstrating the advantages of longer release times. For instance, in 2009, Davies-Venn and colleagues showed that fast acting compression benefits audibility for soft sounds, but degrades conversational and loud speech for people with severe loss. Cox and Xu (2010) also determined that elderly people prefer a longer release time, probably because of the lack of contextual cues, and also because of their lower cognitive level. Similarly, Souza and Sirow (2014) showed that older people or those with more severe loss do better with a slower/longer release time, whereas people with better cognition do better with a faster compression system. With regard to sound quality, a longer release time is better; from an audibility standpoint, a shorter release time or fast release time may be better.
Time Constants
Let's look at how attack and release times are determined, and what they really mean. Figure 5 shows a pure tone signal. Time constants are reported based on a single, sinusoidal signal. The signal in Figure 5 goes from 50 dB up to 80 dB for a period, and then it goes down to the original level. When it is applied to a linear hearing aid that provides 30 dB gain; we know that all inputs are increased by 30 dB. If we apply the same signal to a compression system, after it has been amplified, it goes up to 100 dB, so there is a gain of 50 dB.
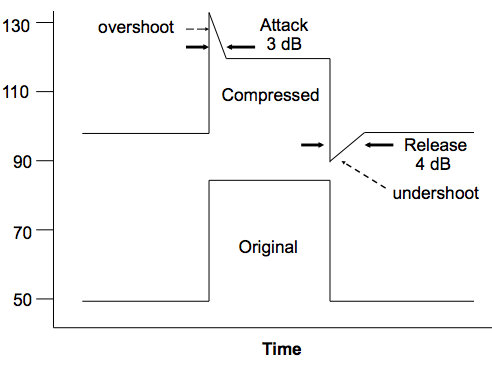
Figure 5. How time constants (attack and release times) are measured.
That 50 dB gain would have brought the 80 dB sound to 130 dB output level; but because of compression, it reduces gain to a steady gain state of approximately 120 dB. Part of the amplified sound initially reaches 130 dB, but quickly falls down to the steady state level of 120 dB; this is what we call the overshoot, or the attack time. This is the time it takes to reach a steady gain state.
When the hearing aid is in the steady state and the input level decreases, the output of the hearing aid also decreases. Because everything takes some time to work, the input level, even though it is 50 dB, still carries the gain of the compressor, or the reduced gain state. The time it takes for the hearing aid to go from the reduced gain state, (which is labeled as the undershoot in Figure 5), back again to the linear gain state or the higher gain state, is the release time of a compression hearing aid.
To illustrate attack and release time, I like the analogy of speeding on the freeway at 100 miles per hour and seeing a highway patrol car in the rear view mirror. Of course, our instinct is to slow down and immediately apply the brakes so that we will comply with the speed limit. The time it takes you to move from 100 miles per hour down to 75 miles per hour is what we call the attack time of the system. It's how much time it takes you to get to the reduced gain. It usually has to be a short timeframe, because you don't want to get a ticket. On the other hand, once the officer is gone, you might say, "Well, I like the thrill. I'm going to drive at 100 miles per hour again." The time it takes you to let go of the brake and hit the accelerator, to go from 75 miles per hour back to 100 miles per hour, is the release time of the system. That dictates how quickly you get back.
The speed of the release time is quite variable. If for instance, my wife is pregnant and I’m taking her to the hospital; obviously, I will want to have very short release time so that we can get to the hospital as quickly as possible. In the process of doing that, imagine that I hit the accelerator very quickly, giving an instant bump, the feeling of a sudden change. On the other hand, if I’m taking a leisurely Sunday drive where I am enjoying the scenery, I might want to have a longer release time. In that case, the release time can be longer. There are no fixed criteria on what a release time should be (whether it should be fast or long), because each one has its own story to tell. Each one has its advantages and limitations.
Fast Acting Compression
Advantages
Speech varies in intensity level over a wide range, from 0 dB to as much as 130 dB. The rationale behind using a fast-acting system is based on a loudness normalization process. We know that hearing-impaired people have a reduced dynamic range. For example, if someone has a 50 dB hearing loss, they may have a dynamic range that is reduced from 100 dB to 50 dB.
The rationale is, if the compression system can go in and out of compression very quickly, then we can capture this full range of 130 dB into the reduced dynamic range of the hearing-impaired individual of 50 dB, for example. When you have a system that is intended to capture a large range of sounds into a reduced dynamic range, you may think it is better to have a system that is acting as fast as possible.
Example – Short Attack and Release Times / Fast Compression System
Let’s look at an example of what happens to a signal in a hearing aid with a fast acting compression system (Figures 6 & 7). In Figure 6, we have a static input/output curve of the hearing aid in black, and then we have the dynamic input/output curve of the system in red. This system has very short attack and release times.
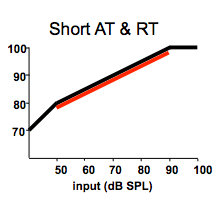
Figure 6. Static (black) and dynamic (red) input/output curve for a system with a short (fast) attack and release time.
In Figure 7, the unamplified signal is shown on the left. The unamplified signal starts at 40 dB, goes up to 80 dB, is silent for a period, and then goes up to 60 dB. It has a peak-to-peak difference of 20 dB. Figure 7 on the right is the same signal amplified by the hearing aid with 30 dB gain, and a 2:1 compression ratio.
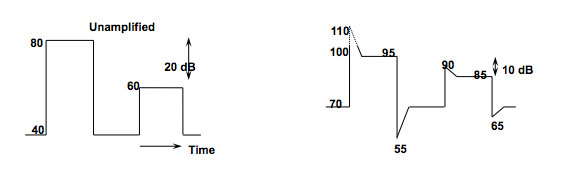
Figure 7. On the left: Unamplified signal. On the right: the same signal amplified per the input/output curve in Figure 6 using a hearing aid with 30 dB of gain and a 2:1 compression ratio with a fast attack and release time. The peak-to-peak difference in the amplified signal is reduced as compared to the unamplified signal.
The output of the amplified signal goes from 70 dB (40 dB signal + 30 dB gain) to 110 dB (80 dB signal + 30 dB of gain), and then very quickly goes down to 95 dB due to compression. Then when the input is less (due to the silence in the signal), the output drops to 55 dB, but it quickly recovers to 70 dB. It then goes to 90 dB, falls to 85 dB, and so forth. In this fast-acting system (i.e., fast release time), you can see the peak-to-peak difference of 20 dB in the unamplified signal is now reduced to only about 10 dB. That is important to recognize.
The second thing that you will see is that the noise level of 40 dB in the original signal recovers to 70 dB in the amplified signal very quickly. One very important advantage of a fast-acting system is that because of the fast gain recovery, audibility of soft sounds is much better than with a system that recovers more slowly. Therefore, audibility of soft sounds is an advantage of a fast acting compression system.
Disadvantages of Using Only Fast Acting Compression
One disadvantage of a fast-acting system is that it reduces the temporal cues, as I mentioned earlier. That is, the peak-to-peak difference of 20 dB that we saw in the original signal is now reduced to only 10 dB. This is more problematic for people with cognitive issues and severe loss, because they rely on the temporal cues much more than people without these kind of issues. This is especially evident when you have a system with a high compression ratio (typically more than 3:1). That is one reason why most hearing aids on the market today would have a compression ratio smaller than 3:1, with many around 2:1. That is primarily because they do not want to exaggerate the smearing of the temporal waveform. This occurs even more so in a multi-channel compression hearing aid, because each one of these channels would be acting independently. You can imagine if you give a lot more gain in a much shorter period of time to each one of these channels independently, the smearing becomes more of an issue. That’s why the claim of a 6,000 channel type hearing aid cannot be true. In reality, you cannot have so many channels working independently, especially with a fast-acting system, because that would smear the temporal waveform, making it even more flat.
Another disadvantage is that ambient noise becomes more perceptible during the pauses, such as when the hearing aid recovers from the 55 dB level to the 70 dB level. With a fast-acting system, when there are any pauses, such as when you stop talking, the wearer would hear a lot of hissing sounds within the hearing aid, amplifying the room noise. In a moderately noisy background, where the signal-to-noise ratio is not negative, but with a very small positive signal-to-noise ratio, then you can imagine the noise will be amplified more than the speech, reducing the signal-to-noise ratio in those environments. In addition, people report poorer speech understanding in noise with fast-acting systems more than with slow-acting systems. All these are more prevalent in compressors with more channels and a higher compression ratio.
In addition, with a fast-acting system you experience the reduction of interaural cues, which are important for spatial hearing, localization and creating a three-dimensional sound perception. The interaural level difference (ILD) between the two hearing aids provides these cues. Let’s look at an example in Figure 8, where a 70 dB sound is coming from the right side.
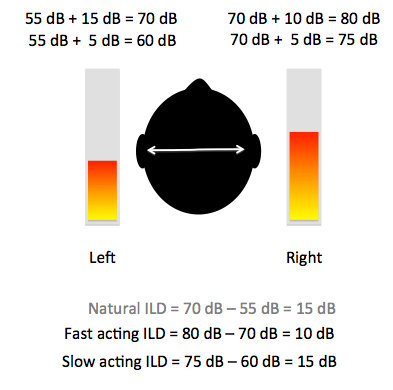
Figure 8. Hypothetical interaural level differences between fast and slow acting compression.
If the sound is 70 dB at the right, because of the head shadow, the sound is 55 dB on the left. With an interaural level difference of 15 dB, we can identify that the sound is coming from the right. Now let’s consider the scenario if both hearing aids have a fast-acting compression system. A fast-acting system would give you the gain as quickly as possible. Of course, we know in a compression system that lower input level means higher gain. In this particular case, when the input to the right is 70 dB, let's say we give it 10 dB gain, and the output is 80 dB. On the left side, since the input is 55 dB, we give it 15 dB gain, and now the output is 70 dB. We can see that the interaural level difference between the left and the right ear is reduced from 15 dB to 10 dB, meaning that we do not have the same ILD difference. That of course may not be optimal for the listener, in terms of knowing the origin of the sound. He will not have the same spatial perception as he has without the hearing aid, or with a linear hearing aid, or in this case, with a slow-acting system. We may allow you to preserve that interaural level difference by giving less gain to the side with the lower input level. That is something that can be done.
Slow Acting Compression
Advantages
Why would people use slow-acting compression? If environmental sounds have level differences of up to 130 dB, wouldn’t that be too much for someone with say, a 50 dB hearing loss? Actually, if we look at any sound environment at any point in time, the level of sound variation is typically less than 30 dB. Pearson, et al. reported this data three decades ago.
They measured the variation in sound pressure level in different environments including: inside home, outside home, school, aircraft, train, as well as when an individual speaks at different levels of vocal effort (casual, normal, raised, loud, shout). They found that there was variation in sound pressure level in these situations, but at any instant in time, and at any vocal effort level, typically the variation in intensity level was less than 30 to 40 dB. That means if a person has a 30 to 40 dB of dynamic range, they can hear the sounds occurring at one particular point in time, or when someone is speaking at a particular vocal effort. In other words, we don't really need compression as long as the gain of the hearing aid is sufficiently high to bring that range of sound into the dynamic range of the patient, and provided that patient has a dynamic range of 30 or 40 dB.
In 1998 Pascoe showed that as threshold increases, MCL increases a little bit, and UCL does not increase as much as the threshold. If we look at the difference between threshold and UCL as a reflection of dynamic range, we find that people with as much as 80 dB hearing loss typically have a dynamic range of 30 dB or more. This means that unless someone has a severe degree of hearing loss, there's no strong need to give them compression, because we can simply take the range of sounds, and move it up into the dynamic range of the hearing-impaired person.
You might ask, "What if the person goes from a soft environment to a loud environment?" Indeed, that is when you would need to have some kind of compression, but it does not need to be happening very fast. You don't change from one environment to another environment instantaneously. That is the rationale for a slow-acting compression system. There is gain change, but it occurs in a longer time span, so that we can preserve the dynamics of the specific situation.
Example - Long Release Time / Slow Compression System
Figure 9 consists of the same static input/output curve (Figure 9 - upper left), and the same unamplified signal from 40 to 80 dB (Figure 9 - upper right) as we used in the earlier example. The amplified signal in Figure 9 (bottom left) is from a slower-acting system. You can see the output goes from 70 to 105, and from 65 to 85 or so. The peak-to-peak difference of 20 dB is somewhat maintained due to the long release time. Indeed, the red curve on the input/output curve shows the effective input/output curve, meaning what the hearing aid doing in the person's ear with a long attack and release time. The static input/output curve (black line) that you see is really not what the patient would experience, depending on the release time and attack time of the hearing aid.
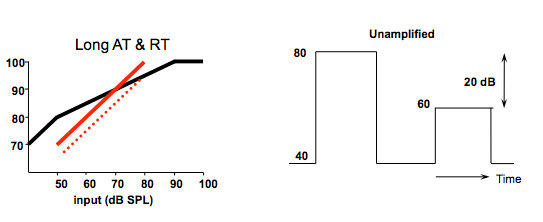
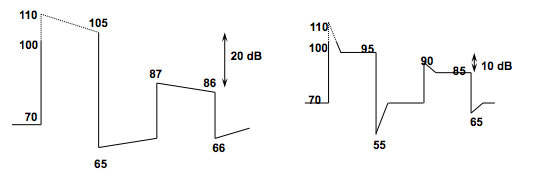
Figure 9. Consequence of a long release time. Upper left – static (black) and effective (red) input/output curve for a system with a long (slow) attack and release time; Upper right – unamplified signal; Lower left – amplified signal with long attack and long release time; Lower right – amplified signal with short attack and short release time.
You can see the difference between a slow-acting system in the bottom left curve of Figure 9, and a fast-acting system in the bottom right curve of Figure 9. With the slow-acting system, there is a 20 dB peak-to-peak level difference, whereas with the fast-acting system, it is reduced to a 10 dB level difference. With the slow-acting system, after the pause between speech it takes a longer time to get back up to the 70 dB level, whereas with the faster system it very quickly goes from 55 dB back to the 70 dB level. In essence, when you have a much longer release time, you linearize the output of the compression hearing aid.
Here is an analogy using happy face emojis (Figure 10). We have a linear hearing aid (represented by the gray line), and a hearing aid with fast acting compression (red line). With a linear hearing aid, amplifying sounds from the soft to loud essentially gives us the same representation of the image on the y-axis, as the original image on the x-axis.
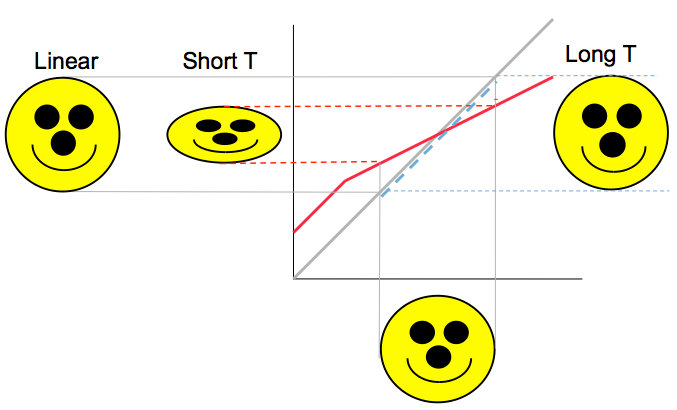
Figure 10. Compression analogy using emoji.
When we use a short attack and release time on a hearing aid, such as the compression system in red, we see the softer sound being amplified to a higher level. The louder sound is amplified to not quite as loud a level as with the linear system. If we plot this on the y-axis, we still see the happy face image, but it looks like it has been squeezed as compared to the original image on the x-axis.
When we change the peak-to-peak relationship of sounds, we alter the supra-segmental cues of the signal. It gives you a different meaning. By using a longer release time, you can see that this linear relationship between the different parts is preserved, and that is the advantage of a slow-acting system. In essence, it acts like a linear hearing aid at any point in time, but over time, the hearing aid does have compression, changing the gain according to the needs of the environment.
Advantages of Using Slow Acting Compression
Advantages of using slow acting compression include:
- Longer release time, less effective compression ratio, more linear – preserve temporal structure
- Preserves short term changes within the envelope (and temporal fine structures)
- Preservation of signal-to-noise ratio in moderately noisy places (Neuman et al., 1998)
- Preservation of natural interaural level difference cue for spatial hearing
- Higher naturalness and better sound quality (e.g., Neuman et al, 1995, 1998; Hansen 2002).
- Better speech intelligibility for people with more than a moderate loss (Souza et al, 2005; Davies-Venn et al, 2009)
Cognition and Release Time
Interestingly, in the last 10-15 years, people have drawn a link between hearing aid processing (specifically the time constants on a compression hearing aid) to cognition. There are many studies demonstrating that people with a lower working memory do better when they have long time constants versus short time constants (Figure 11). Conversely, people with a higher working memory tend to do better with shorter time constants than longer time constants. Other studies have shown that when you improve or enhance the temporal envelope, it improves speech understanding, especially for people with auditory neuropathy spectrum disorder.
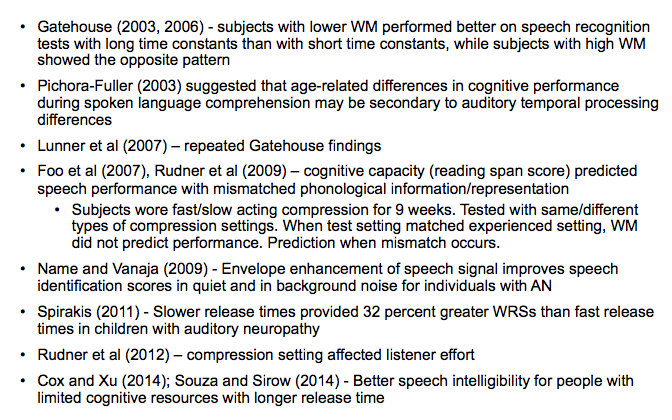
Figure 11. Studies on cognition and release time.
For the sake of time, we are not going to go through each one of these studies. I have, however, summarized the findings using a 2 x 2 matrix (Figure 12). If we look at all these studies, we can make the following conclusions regarding the effects of fast-acting and slow-acting compression on people with good working memory and poor working memory.
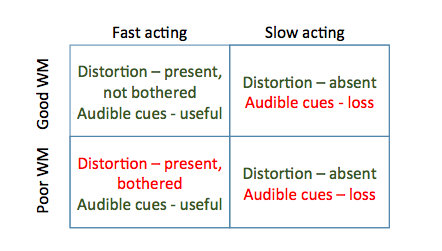
Figure 12. Summary between compression speed and working memory (WM).
With fast-acting compression, we might have distorted the temporal waveform, but we have given people better audibility. People with good working memory are not affected by the distortion. It may not sound quite as clear or natural, but they can understand, and they are not bothered by it. People with good working memory do quite well with fast-acting compression. On the other hand, for the same people, if we give them slow-acting compression, there's no distortion of the temporal waveform. However, especially when you're testing at a soft level, the loss of audibility cues could be detrimental for them, so they do not do as well with slow-acting compression as compared to with fast-acting compression.
For people with poor working memory, a fast-acting system distorts the temporal cues; but since these people are very dependent on temporal cues, it affects their performance. It does give them audible cues, but perhaps the improvement in audible cues is not enough to offset the distortion from the fast-acting system. That's why they may not do quite as well with a fast-acting system. Whereas for the same group of people, when we use a slow-acting system, audible cues are lost, but since the signal is less distorted, and they are more dependent on the temporal cues, they do better than with fast-acting compression.
In essence, we are looking at two factors that are interacting: temporal cues and audibility cues. The temporal cues within the signal (the waveform envelope and the fine structure) are preserved by the slow-acting system. Audibility cues are better with a fast-acting system. How well a person can understand speech is dependent on the interaction between the temporal waveform and the audibility cues.
The question that we have to ask is, if we preserve audibility, would a slow-acting system be poorer for someone with a good working memory? The data that we have seen from Lunner and Sundewall-Thoren (2007) shows that a slow-acting system may not be that bad. They looked at the word recognition performance of people with good cognition and people with poorer cognition in four different scenarios: slow and unmodulated, slow and modulated, fast and unmodulated, and fast and modulated.
As we would expect, when the signal-to-noise ratio improves, performance improves for both groups. With a slow and unmodulated situation, people with good working memory and high cognition do better than the other two groups (poor working memory and intermediate working memory). The same is true whether it is a fast and modulated noise, or a fast and unmodulated noise. In a fast and modulated situation, the intermediate working memory and the poor working memory people do much worse than the people with good working memory.
If we look at the performance of people with good working memory, would they do worse with a slow-acting compression system? At a 0 dB signal-to-noise ratio, the people with good working memory performed at 90% word recognition, regardless of whether their hearing aid processed sound in a fast way or a slow way, and whether it was modulated or unmodulated. This leads us to conclude the following: people with poor working memory are more affected by the temporal waveform. In addition, people with good working memory perform better with a fast-acting system, but they are not negatively affected by the use of slow-acting compression as long as audibility is preserved.
Implications for Hearing Aid Design and Audiology
A knee-jerk reaction might be to presume that we should give fast-acting compression to people with good working memory, and we should give slow-acting compression for people with poor working memory, because they need the temporal waveform. That is true to an extent, but if you look at the data, you can also see that good working memory people are not affected by the slow-acting compression, as long as we give them the same amount of audibility.
We also need to take into consideration some other important factors. All the studies that were being reported were done with one form of compression, meaning that they were conducted with one compressor using primarily fast compression or slow compression. In hearing aids today, we do not use only one form of compression. The findings of the research are valid, but they may not always apply exactly to the implementations of compression used in today’s hearing aids.
Next, we need to consider what sacrifices will occur with each type of compression. When we exclusively give fast-acting compression to people with good working memory, they would get poorer sound quality, even though they can understand speech because they can tolerate the distorted temporal waveform. If we give only slow-acting compression to people with poor working memory, then we compromise the audibility cues. Although the temporal waveform would be preserved, they would be missing out on the audibility cues.
Perhaps the third and practical thing that we need to think about is the issue of how do we classify people into good and poor working memory? As hearing healthcare professionals, that is not our area of expertise or within our scope of practice. In addition, there are no formal tests that can accurately determine if someone has a good or poor working memory. Finally, administering those tests takes time and effort.
Adaptive Compression
If we consider all of the aforementioned factors, then perhaps the best solution for all people, regardless of their memory classification, is if we have a compressor that can preserve the temporal waveform, and at the same time give people the audibility cues that they need. That is something that we have been doing throughout the last 20 years with adaptive compression. In Widex hearing aids, the system primarily uses slow-acting compression. However, when there is a sudden change in the intensity of sound, we invoke the Sound Stabilizer, which changes the release time of the hearing aid so that it can cope with the sudden changes. When sound goes from loud to soft or soft to loud, it can adapt to the sudden changes to provide audibility at that particular point, as well as the temporal waveform at other points in time.
As represented in Figure 13, you see a loud sound followed by the soft sound. Without the SoundStabilizer, the waveform is relatively smaller. With SoundStabilizer, it changes its release time to be much faster so that it is amplified a little bit more. That is what we can do with one compressor using this adaptive control of the release time on the hearing aid.
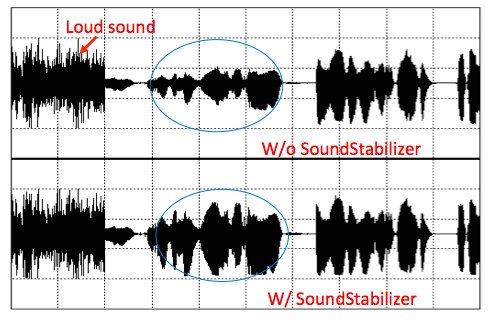
Figure 13. Adaptive compression via SoundStabilizer.
Desirable Enhancements in Single Speed Compressors
What can we do with a compression hearing aid to make it even better? In a system that uses primarily fast-acting compression, we need to preserve the waveforms at all input levels. Fast compression is especially good for softer sounds, so the limitation here is what do we do with conversational and louder sounds to preserve the waveform? If on the other hand, you have a system that uses primarily slow-acting compression, what would you do to preserve the audibility for the softer sounds, or the transition from the low gain to the high gain?
The ideal solution is having two compressors. What we have been doing all along is using one compressor and changing the speed adaptively. Now with advancing technology, we can use two separate compressors: one working as a slow-acting compressor (primary), and another fast-acting compressor working in parallel so that we can preserve the temporal waveform as well as the audibility cues of the system. Figure 14 shows a schematic illustration of such a system.
Figure 14. Variable speed compressor. The overall input gain equals the slow acting compressor (SAC) gain plus the fast acting compressor (FAC) gain.
With one particular channel, you can see that the signal is split so that it goes to a slow compressor (SAC), which determines the overall gain of the hearing aid. Another branch of the same signal goes to a fast compressor (FAC) so that it can be working on shorter-term fluctuations of the signal. The output from the faster compressor and the slow compressor is added together to give you the output at that particular channel. This is the principle behind a variable-speed compressor: two compressors working at the same time in each one of the different channels, and the output determines what the hearing aid gives out.
Effortless Hearing
This is the design rationale behind the Widex UNIQUE variable-speed compressor that we call Effortless Hearing. That is, we use the compressor so that regardless of your cognitive background, whether you have good or poor working memory, you can realize your potential, and the signal will be as clean and as audible for you as possible. We use two compressors working in the manner that I just demonstrated. The important thing in this case is how these two compressors work. The algorithm behind the compressor is what dictates how well this dual compressor will work.
Figure 15 shows a signal that goes from very soft to very loud, and the gain that results from a single speed, slow compression system. With a slow compression system, the gain is relatively high when the speech level is low, and then when the speech level is higher, the gain decreases. You don't see a lot of fluctuation with a slow compressor.
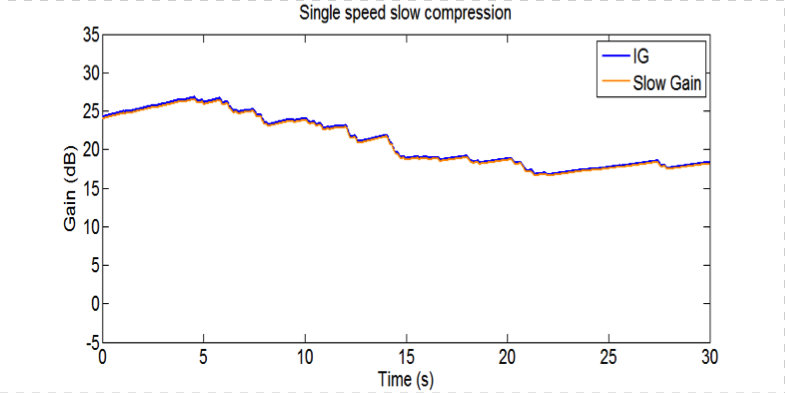
Figure 15. Single speed slow compression.
Figure 16 shows the same speech signal going through a single speed, fast compressor. You can see a lot of fluctuations in gain. A fast compressor applies gain constantly to the signal at every point in time.
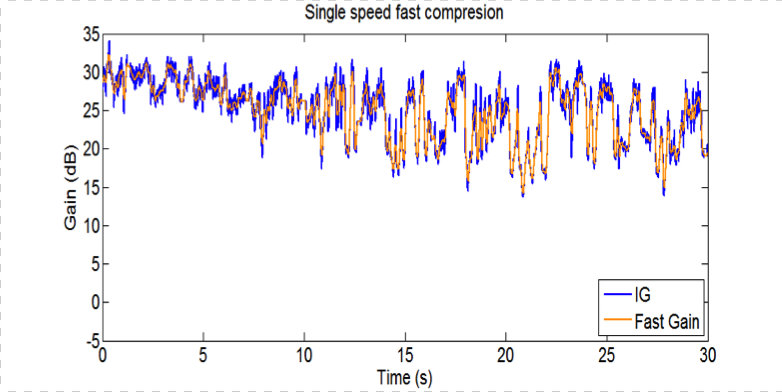
Figure 16. Single speed fast compression.
Figure 17 is a dual compressor, with a fixed speed. The red line is the gain that the fast compressor provides, and you can see in this particular case the gain is very little, but it does change a lot with the input level. The orange line is the gain for the slow compressor, which is much higher gain, but the gain level doesn't change. It's the summation of the orange line and the red line that gives you the overall gain of the hearing aid in this fixed speed, dual compressor.
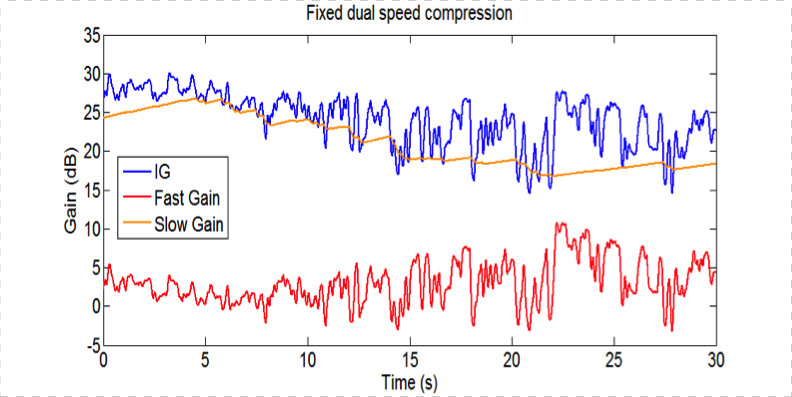
Figure 17. Fixed dual speed compression.
Figure 18 shows a variable-speed compressor. You can see that there is gain variation but it is much less. That follows the change in the fast compressor. That is the principle behind a variable-speed compressor.
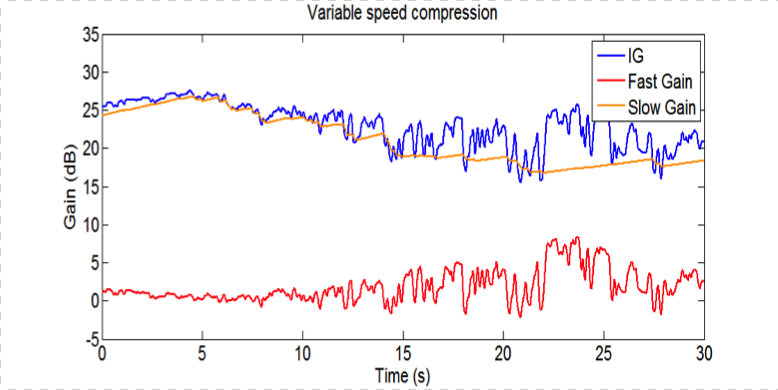
Figure 18. Variable speed compression.
Additional Measures to Minimize Temporal Smearing
We have a slow gain compressor, a fast gain compressor, and we add them together. What can we do to further minimize any temporal smearing of the signal? First, because slow-acting compression preserves the temporal waveform, we use it as the primary compressor, and it determines the overall gain of the hearing aid. We only use fast-acting compression as needed in very specific situations. We do not use it a lot, because we still think the temporal waveform is important, but we are adding the audibility cues to the extent that doing so would not affect the temporal waveform.
One measure to minimize temporal smearing is to use modulation control. Modulation control measures the modulation characteristics of the input signal. When it is very low modulation, we will not provide fast compression; if the modulation is high, we can give the signal a little bit of fast compression. It reduces the peak, but it would not reduce it as much when the signal is present in a quiet situation. In a quiet situation, we give you some fast acting compression, but when it is noisy, we are not going to give it to you because the signal-to-noise ratio is already poor.
We know from the studies on channel bandwidth, that the more channels we have, the more likely the signal will be smeared. Figure 19 shows the formants of a particular signal. The blue line is that of a linear hearing aid; the red line is a two-channel system, and the green line is that of a ten-channel system. You can see that a ten-channel system reduces the peak-to-peak difference, but a two-channel system preserves some of that. If we can effectively reduce the number of channels in a hearing aid, we can reduce the amount of temporal smearing on the signal.
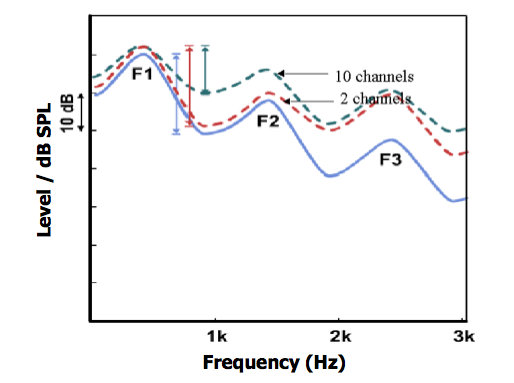
Figure 19. Spectral smearing.
Figure 20 shows the envelope of a linear hearing aid with both a narrow (15 channels) band and a wide band (3 channels). The slow-acting system (left) preserves the temporal waveform envelope quite well. With a fast-acting system (right), you can see the difference between the 3 channel system (light blue line) and the 15 channel system (green line). Again, if we can effectively reduce the number of channels, we can better preserve the temporal waveform.
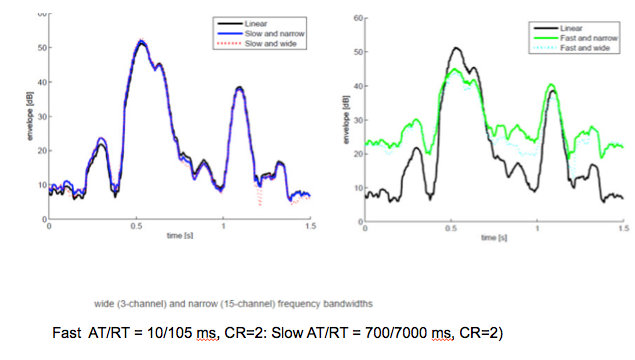
Figure 20. Effect of channel bandwidth and release time on temporal envelope.
With the Widex UNIQUE hearing aid, we link the nearby channels. For example, rather than have the output of one channel be used as the overall output, we link the output of the channel before it and the channel after it; we then take the average of all three channels with the fast-acting compressor to add to the slow-acting compressor. By linking nearby channels, we can reduce the amount of temporal smearing on the signal, and that preserves the waveform.
We also consider the effect of the compression ratio on temporal cues. A higher compression ratio means there is less of an intensity difference between sounds and therefore more temporal smearing. When we have a high compression ratio, the peak-to-peak difference is poorer than when you do not have quite as high a compression ratio in the system.
We know that people with a severe hearing loss depend on the temporal waveform. For people with a severe hearing loss, our system does not give as high of a compression ratio in order to preserve the temporal waveform as much as possible. It enhances audibility, but it does not distort the temporal waveform quite as much. A variable-speed compression system gives you that advantage: it preserves the temporal waveform as much as it can, with minimal distortion. It restores the audibility that a fast-acting system allows you to have when there's a change in the level of sounds from soft to loud and from loud to soft. We did a study where we had a loud sound followed by a soft sound, and we detected the audibility of that soft sound. We found that our variable-speed compressor outperformed even our SoundStabilizer system, which already uses an adaptive compression system.
The advantages of a variable-speed compressor over a single-speed compressor are summarized as follows:
- More consistent audibility for soft sounds, especially after a loud sound.
- More comfort for transient sounds, and when transitioning from soft to loud sounds.
- Better signal-to-noise ratio at high input levels, preserving the temporal structures (and better speech understanding in noise).
- Better preservation of temporal waveform at all input levels.
- Optimal for people with good and not-so-good working memory and those with severe hearing loss.
Conclusion
The speed of a compression system has important consequences on wearer success. No system is using an exclusively fast or exclusively slow compression system. This is primarily because we know that a fast system gives you extra audibility, but it creates temporal distortion; a slow system preserves the temporal nuances, but it has the potential of some loss of audibility. Therefore, if implemented properly, a variable-speed compression system has the advantage of giving you the benefit of both systems, and limiting the disadvantages of either one. A variable-speed compression system that preserves temporal structures and audibility cues may be desirable for all people, whether they have good or poor working memory.
Questions and Answers
Why do individually acting channels produce temporal smearing?
Temporal smearing happens when each channel in a hearing aid works independently. If we have a single channel system (e.g., from 100 Hz to 10,000 Hz), the gain of that system is the same. The compression ratio and everything is the same. If we apply 15 dB gain to it, that 15 dB gain would be the same for 1000 Hz, 2000 Hz, and 3000 Hz all along the signal. When you look at it this way, then everything is given the same amount of change so the waveform or the peak-to-peak differences are more preserved.
Consider a 4-channel system where you have the following:
Channel 1, < 1000 Hz
Channel 2, 1000 – 2000 Hz
Channel 3, 2000 – 4000 Hz
Channel 4, >4000 Hz
In this kind of a system, you can apply different amounts of gain in the various channels. Typically, because most people have more hearing loss in the high frequency, we give them more gain in that region. In this example, let’s say that the hearing loss is such that you give them 30 dB gain in Channel 4, and 20 dB in Channel 3 and 10 dB gain in Channel 1. The 40 dB gain added to the high frequency may give you an output that is similar to the 30 dB gain added to the mid frequency, and similar to the 10 dB gain added to the low frequency. When you have more channels acting independently, everyone is doing its own thing without any communication with the other channels. Then the differences between the various areas of the signal (peak-to-peak differences) are reduced.
If you link nearby channels, then whatever the middle frequency does will still need to communicate with the lower frequency or the higher frequency, for example. That is one way of reducing the effective number of channels. Linking the channels or reducing the number of channels in a hearing aid is a way to preserve temporal smearing.
Is there is a preference for keen music listeners, whether there's a fast or slow-acting compression?
Whether people have a music background or not, people prefer the slow-acting compression for music precisely because it keeps the temporal differences between one frequency and the other frequency. People with music background tend to prefer the slow-acting compression more than a fast-acting compression, if the hearing aid has to use compression. These people like the single-channel system better than a multiple channel system because of the level differences that it would preserve.
What do you recommend for a profound hearing loss with less than 20 dB dynamic range?
Typically, for people with profound hearing loss, you want to use as slow a compression as possible, or as linear of a hearing aid as possible. On the other hand, you would recognize that this would obviously compromise some audibility cues. They will need temporal cues much more than the spectral cues so you may sacrifice on that, but your best bet is a slow-acting compression. The Widex Unique has a much more slow acting compression than any of our other hearing aids to date.
In hearing aid programming, when you make changes between audibility and comfort in the sound class settings, are you also altering the variable-speed compressor?
At least in our software, we are not altering the variable-speed compressor when you change from comfort to audibility. We are changing the noise reduction features that you adjust, as well as the gain parameters. The noise reduction might be more active or less active, or the directional mic might be more active and less active in this case.
References
Cox, R. & Xu, J. (2010). Short and long compression release times: Speech understanding, real-world preferences, and association with cognitive ability. J Am Acad Audiol, 21,121–138.
Davies-Venn, E., Souza, P., Brennan, M., Stecker, G.C. (2009). Effects of audibility and multichannel wide dynamic range compression on consonant recognition for listeners with severe hearing loss. Ear Hear, 30(5), 494–504. doi: 10.1097/AUD.0b013e3181aec5bc
Hansen, M. (2002). Effects of multi-channel compression time constants on subjectively perceived sound quality and speech intelligibility. Ear Hear, 23, 369–380.
Lunner, T. & Sundewall-Thoren, E. (2007). Interactions between cognition, compression, and listening conditions: effects on speech-in-noise performance in a two-channel hearing aid. J Am Acad Audiol, 18(7), 604-17.
Neuman, A.C., Bakke, M.H., Mackersie, C., Hellman, S., & Levitt, H. (1995). Effect of release time in compression hearing aids: paired-comparison judgments of quality. J Acoust Soc Am, 98(6),3182-7.
Neuman, A.C., Bakke, M.H., Mackersie, C., Hellman, S., & Levitt, H. (1998). The effect of compression ratio and release time on the categorical rating of sound quality. J Acoust Soc Am, 103, 2273–2281.
Pascoe, D.P. (1988). Clinical management of the auditory dynamic range and their relation to the formulas for hearing aid gain. In J.H. Jensen (Ed.), Hearing aid fitting: Theoretical and practical views (pp 129-152). 13th Danavox Symposium. Copenhagen, Denmark: Stougarrd Jensen.
Souza, P., & Sirow, L. (2014). Relating working memory to compression parameters in clinically fit hearing aids. (2014). Am J Audiol, 23(4), 394-401. doi: 10.1044/2014_AJA-14-0006
Further references are included in the course handout.
Citation
Kuk, F. (2016, September). Selecting the right compression. AudiologyOnline, Article 18120. Retrieved from www.audiologyonline.com