Learning Outcomes
After this course, participants will be able to:
- Explain why over-amplification is not a concern with a SuperPower BAHS device.
- Describe who can benefit from a SuperPower sound processor.
- Explain in which directional mode the speech intelligibility is improved with FreeFocus.
- Describe how SuperPower is fitted and what reactions to expect from patients.
- Describe what FLogram is and what it can be used for.
Introduction
The Ponto 3 family includes three products: the Ponto 3, the Ponto 3 Power, and the Ponto 3 SuperPower. The SuperPower product is the first product available to be fit on abutment level, with a fitting range up to 65 dB HL. The Ponto 3 family is the definition of power, making listening and participation easier with the introduction of BrainHearing, with our powerful sound quality, and our reliable performance.
For the first time, we are pleased to introduce BrainHearing in bone anchored devices. BrainHearing is about making it easier for people to listen, requiring less effort to participate in conversations. BrainHearing is our guiding star, and we have two evidences for BrainHearing. First we have evidence from a study that shows that direct sound transmission makes it significantly easier to recall words, as opposed to skin-drive solution – a softband solution (Lunner, Rudner, Rosenbom, Ågren, & Ng, 2016). Additionally, research has shown that our new directionality feature, FreeFocus, provides users with a 15% better speech intelligibility, 70% of the time (Oticon Medical, 2016; Wagener, Josvassen, & Ardenkjær, 2003). The powerful sound quality is characterized by the highest output ever in an abutment level sound processor. Furthermore, all Ponto products have the widest frequency bandwidth available on bone anchored devices (up to 9.5 kHz). High frequency audibility is important for speech and language development.
Participation is easier than ever, thanks to the wireless streaming possibilities and reliable performance of the Ponto 3 family of products. You may be familiar with our Streamer solution from Ponto Plus (Bosman, Hol, Snik, & Mylanus, 2014; Bosman, Mylanus, Hol, & Snik, 2016). Now, we also have included binaural synchronization and coordination. In other words, in any binaural fitting, the left and the right devices will align (the noise reduction and the directionality mode). In addition, if the patient operates the volume control or change program on one side, it will be transferred and also adjusted on the other side. Lastly, we are empowering children with our products that now include not only a new Ponto Softband, but also for the first time, the DSL fitting rationale, tailor-made for bone anchored devices (Hodgetts & Scollie, 2017).
Challenges in Bone Anchored Devices and Who Can Benefit from SuperPower
A constant challenge with bone anchored devices is the maximum force output level of the devices. We know from studies that the loudness discomfort level (LDL) for a conductive hearing loss, when measured with bone conduction typically is around 95 dB HL. We also know that the maximum force output of bone anchored devices is fairly low.
Figure 1 shows the maximum output for various devices as measured in dB HL. These values were compiled by Ad Snik, and published on his blog called Snik Implants (www.snikimplants.nl). It's a very comprehensive and detailed blog that I highly recommend, if you want to know more on bone conduction devices. This table compares the objective measurement of the maximum power output (MPO) of several hearing devices. Up to around 80 dB HL is the most powerful bone anchored device. We can see that the maximum power output of the Ponto device is well below the loudness discomfort level of the patients.
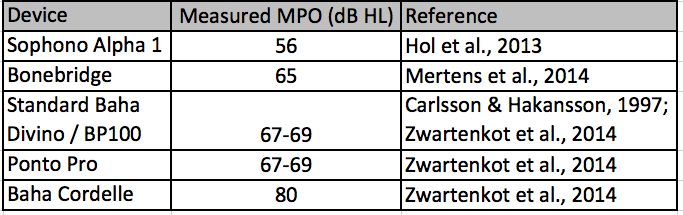
Figure 1. Objective measurement of the MPO of several hearing devices, adapted from www.snikimplants.nl
Ever since we introduced the first Ponto Pro device in 2009, we have increased the maximum output with the launch of each new product. Now, we have the SuperPower product that, compared to the first product we launched, has a 14 dB higher maximum force output (Figure 2). This is the highest output ever from an abutment level sound processor.

Figure 2. MFO for Ponto Pro, Ponto 3, Ponto 3 Power and Ponto 3 SuperPower, the MFO is increased by 14 dB in the high frequency area.
Ponto 3 Family Fitting Range
Ponto 3 has a fitting range up to 45 dB HL; the Ponto 3 Power, up to 55 dB HL; and the Ponto 3 SuperPower, up to 65 dB HL. When looking at this fitting range (Figure 3), one might conclude that the SuperPower product is a niche product only for the patient with a large mixed hearing loss. However, we need to focus more on what is the implication of using devices with different maximum force output; to start discussing what is the lower limit of using the product. We have indicated the maximum limit, but the interesting question is, what is the minimum limit at which it is appropriate to use the SuperPower device?
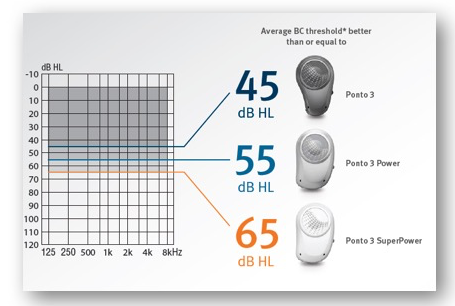
Figure 3. Ponto 3 family fitting range.
In Figure 4, the thin, green vertical line represents the input level, and the orange line to the right represents the output level. Imagine that we have a patient with a conductive hearing loss, and we are fitting that patient with a device with a certain maximum force output. The patient is going to have a certain amount of amplification (indicated with the black lines). For a certain input level, you have a corresponding output level that is higher. As the input level increases, the output in the device increases, but at some point, the output will not increase to the same degree. In other words, the output has hit the ceiling, or the maximum force output of the device, as indicated by the red bar. In Figure 4, we can see that saturation occurs at the input level indicated by the smallest green arrow. That means, any input higher than the saturation level will not be perceived at a higher level for the patient. The input levels up to the saturation level shows the dynamic input range that the patient can listen to, where the sounds are reproduced at a higher loudness level. Any input higher than the wide green bar is not perceived louder for the patient.
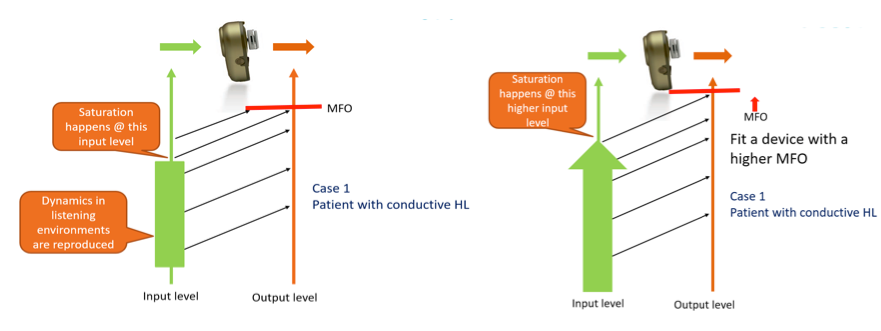
Figure 4. Illustration of input, output and saturation. The input dynamic range, that is reproduced naturally, is increased when using a device with a higher MFO as shown to the right.
Looking at a different scenario, let's fit the patient with a higher MFO device (right part of Figure 4). In that case, we see that the saturation level increases. Because a higher MFO is still below the patient's loudness discomfort level, that means that the patient is able to access to more sounds coming into the device, without distortion caused by the maximum force output when it hits the ceiling. What the patient perceives is a larger proportion of the dynamics, in the environment and the speech spectrum, are reproduced without being limited.
What is the effect of higher max output? We know from a previous study comparing the Ponto Pro and the Ponto Plus, that the sound quality increase was significantly better using the device with the higher MFO (Bosman, Hol, Snik, & Mylanus, 2014). Data can be seen in Figure 5.
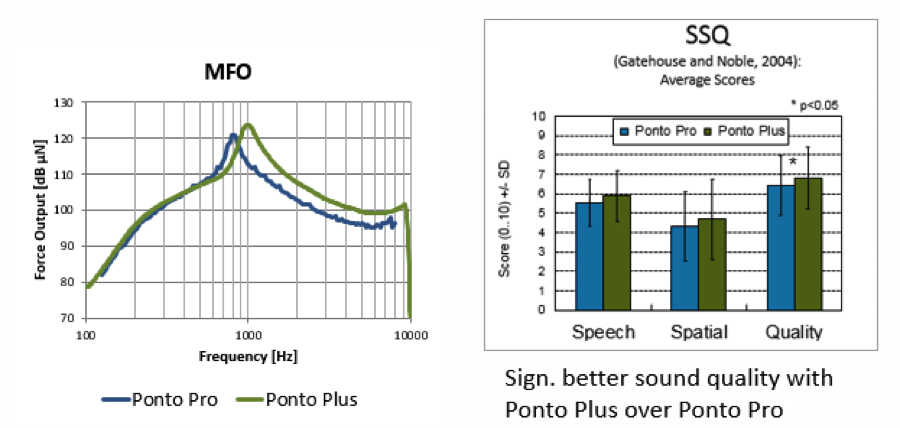
Figure 5. Study comparing two devices with different MFO for a group of patients with conductive and mild mixed hearing losses, showed signification better sound quality with the device with higher MFO. From Bosman, Hol, Snik, & Mylanus (2014).
Patients Who Need More Gain
There are several reasons why patients might need more gain in their device. It may be because they have a larger hearing loss, it can be because they are fitted with advice on a Softband, alternatively they are an SSD patient. In those cases, the patients need more amplification, as illustrated here with the blue lines (Figure 6). As we increase the input level, we see that we reach saturation at a lower input level. In this case, when we fit a device with a higher maximum force output, we can then increase the saturation level, so that it comes closer to that of patients with conductive hearing loss.
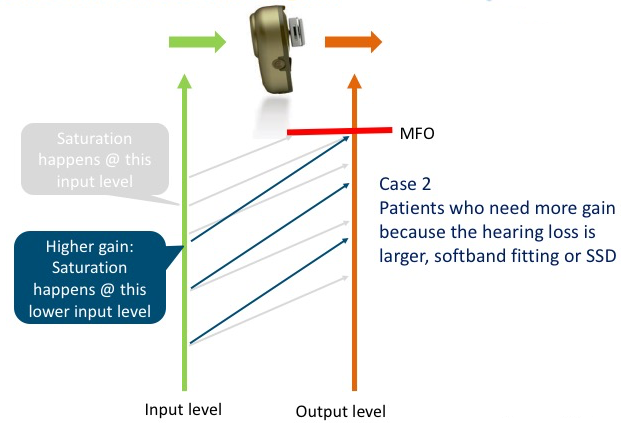
Figure 6. Patients who need more gain.
In a Softband solution, we provide higher amplification to overcome the dampening via skin and tissue. We can therefore use the case from above (Figure 6) to illustrate what happens in a softband case. In Figure 7, the effect of the skin dampening is shown to the right.
The perceived maximum output on abutment (indicated by the orange vertical arrow) is lower because of the attenuation via the skin and tissue. The attenuation is illustrated by the downward blue arrows.
In a Softband solution, we are providing more amplification, because we want to ensure that the final perceived output level on a Softband is equivalent to how it would be if it was perceived on an abutment. But we have to realize that in Softband or magnetic solutions, is that the perceived maximum force output is lower compared to how it is on abutment. There's nothing we can do about the level of the max output level, we increase the gain; but it doesn't affect the maximum force output. The perceived maximum force output of a device fitted on a Softband or a magnetic solution, will always be lower as it is compares to an abutment solution.
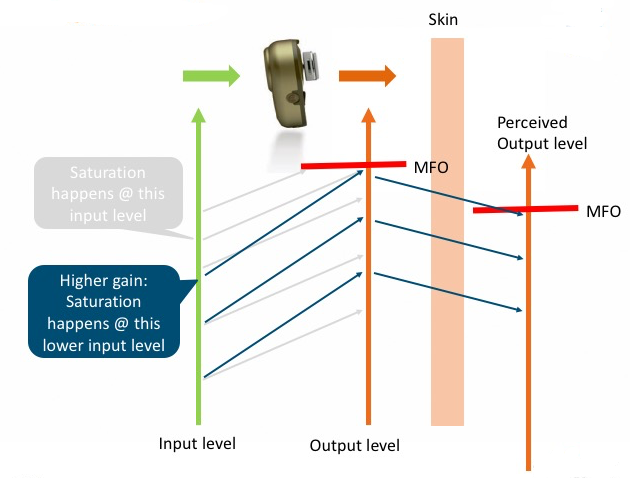
Figure 7. Case from Figure 6 is applied on a Softband solution. The perceived MFO on softband (to the right) is lower compared to abutment (mid line).
In summary, which patients are the best candidates who can benefit from Ponto 3 SuperPower?
- Patients with conductive loss. A higher MFO means better utilization of patient’s dynamic range. These patients have normal cochlea; the higher the MFO we provide these patients, the more natural sounds can be produced in louder listening environments.
- Patients with mixed hearing losses. A higher MFO gives these patients a larger dynamic range (a.k.a., headroom in the device), so more sounds are reproduced naturally without being limited. When we fit mixed loss patients with Ponto 3 SuperPower, it is because we need to provide more amplification. Of course, due to the higher gain, we would then need to have an excellent feedback management system.
- Softband and head band users. If we fit SuperPower devices on Softband or head band users, they will benefit greatly from using a product with a higher MFO, due to the skin attenuation (sound dampening). If we use a product with a higher MFO, the sound will be closer to what it would be if we used a device on abutment. Still, we must remember that whenever we fit a device on Softband, the perceived maximum force output is lower than on abutment.
- SSD patients. When we use the SuperPower device for patients with single sided deafness, they will have better ability to loudness match sounds from the device to the normal hearing ear.
One might argue that we should recommend a SuperPower device to all patients. However, we would never use a SuperPower BTE device to treat mild sensorineural hearing loss; that would result in “over-fitting” the patient. It stands to reason then that audiologists might hesitate to use a SuperPower device for small losses. But that doesn't count for bone anchored devices, because as we have seen, the maximum force output in the device is well below patients' loudness discomfort level. We also know from traditional hearing aids, if we were to fit a SuperPower behind the ear device to a patient, the fitting software will give us a warning to indicate that we are fitting a high-power instrument. We never receive that warning when we fit bone anchored devices, because we are not exceeding the patient’s loudness discomfort level.
Additionally, if we are fitting smaller losses, you may question whether the gain prescribed is low enough. In fact, it is, because we are prescribing exactly the same amount of amplification to patients with conductive hearing loss using a small device as we would if we were using a SuperPower device. There is no risk of overamplification when fitting the SuperPower device for a patient with a conductive loss or mild mixed loss. Also, you can assure the patient that when they use the volume control, that maximum that they can turn up the volume is 10 dB. That way, there is no risk that they can give themselves too high gain.
Allow Patients to Test SuperPower
It is not likely that a patient will come in to the clinic and ask to have a SuperPower device. It is our responsibility to inform all bone anchored patients about the benefits of having higher maximum output. Our advice is to let the patients try the SuperPower device. Let them use the device to experience different dynamic environments (walking outside on the street, around the hospital, in the clinic). That way, they can hear the sound quality and clarity of the device. It's all about giving the patient information, so that they can make a balanced and informed decision about which device they want to use. When patients come into the clinic and select a device, there are certain characteristics that are very tangible, and easy to see and feel (e.g., the cosmetics of the device, the handling of the device, what kind of wireless system is in the device). Other aspects, such as speech intelligibility and sound quality, are not tangible. The patient will not know that there can be differences between products unless they try them, and we inform them.
Ponto 3: Sound Quality
Sound quality is a factor that is determined by many different aspects. One important ingredient for good sound quality is high output. Having a wide bandwidth is also important, and results in a greater range of high and low tones. Additionally, a key element to sound quality is clarity without distortion. Our directionality system can bring clarity into listening situations, so that listening becomes easier. Those of you who have fitted Ponto devices likely know that all our products are known for excellent sound quality, and the Ponto 3 family is no exception.
FreeFocus Directionality System
The new directionality system in the Ponto 3 products is called FreeFocus. In addition to split and full directional modes, the FreeFocus directionality system introduces a new FreeFocus mode: Speech Focused. Furthermore, it is an automatic directionality system.
Automatic Directionality
All Ponto devices have automatic directionality, and will automatically change between being in surround, split and full directionality modes. The device automatically selects the mode that will provide the best signal to noise ratio, based on the existing sound level in the environment.
With all automatic directionality systems, we have to bear in mind the proportion of time that these devices are in surround, split and full directionality mode. In a study of twenty people who used a Ponto device for a few days, the breakdown of time spent in each mode is as follows:
Surround Mode = 79%
Split Directional Mode = 15%
Full Directional Mode = 6%
There were variations among paticipants, but the majority of the time, the subjects’ hearing aids were in surround mode (Oticon Medical, 2016). This is because if the devices switch to full directionality or split directionality mode for larger proportion of the time, the patients would find the devices too weak, or they might be able to hear noise from the microphone. In general, apart from this sample of people, surround is the mode used most often (at least 70% of the time).
With the FreeFocus directionality system, we looked into whether we could improve speech intelligibility during that 70% of the time when hearing aids are in surround. If we can make listening easier in the majority of situations, then the patient spends much less energy on listening, thereby supporting the BrainHearing aspect of the devices.
In Figure 8, you can see the distribution of the directionality. This is a screen shot of the fitting software in Genie Medical for a specific patient. In this example, the patient has been in Surround mode 71% of the time.
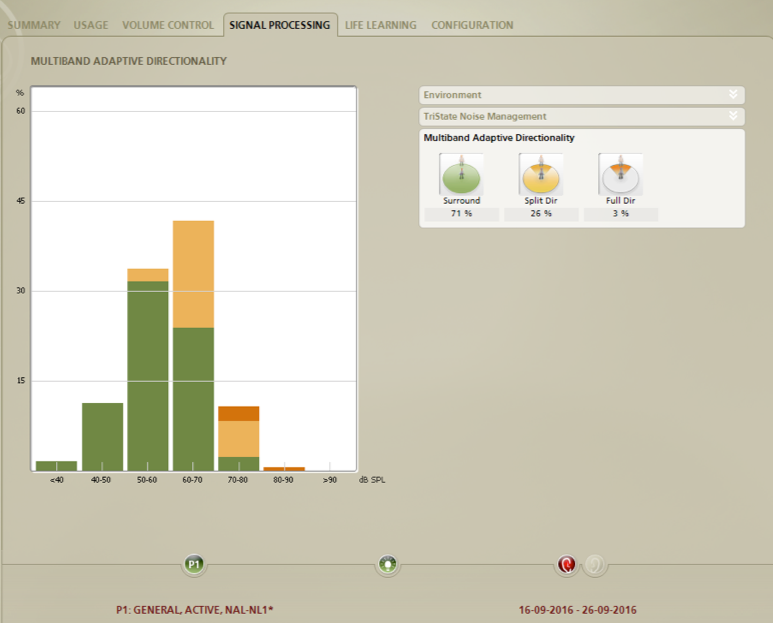
Figure 8. Sample of multiband adaptive directionality, and the distribution in Surround (71%), Split-Directional Mode (26%) and Full Directional (3%).
Speech Focused Mode
The new Surround mode in Ponto 3 devices is called Speech Focused. It has a light directional mode for frequencies above 1880 Hz. This keeps the lower frequencies omnidirectional, allowing environmental input from all directions, and high frequencies in a more directional mode, to enhance focus on the source of interest when positioned in front of the listener.
Evidence
We conducted a study to compare the subjective and objective outcome of the FreeFocus directionality system in Ponto 3 to the directionality system in the previous generation, Ponto Plus (Oticon Medical, 2016). Our subjects included 19 adult patients with varying degrees and types of hearing loss (conductive = 5, mixed = 9, single-sided deafness = 5). They all tested Ponto 3 with FreeFocus in their daily listening situations. Patients that were accustomed to having a Ponto Plus device were fitted with a Ponto 3 device. Patients accustomed to using a Ponto Plus Power device were fitted with Ponto 3 Power. The SuperPower device was not part of this test, because we wanted to focus alone on the FreeFocus aspect.
We found that when we measured the speech intelligibility in the laboratory, we saw a 1.1 dB improvement in the signal to noise ratio when using the Speech Focused mode in Ponto 3, as opposed to the Ponto Plus’ Surround mode. That improvement of 1.1 dB is equivalent to 15% improved speech intelligibility with the speech material that we used (Wagener, Josvassen, & Ardenkjær, 2003).
In daily listening environments, patients were using the automatic directionality. That means, depending on their environment, the device would change between the surround, split and full directionality. When they came back and rated the functionality of the directionality system in daily life, we saw a significantly higher score for speech understanding with Ponto 3, as well for the spatial aspects.
Patient Comments on Ponto 3 (FreeFocus)
Our objective findings from the laboratory were in line with the subjective experiences of these patients. In general, patient comments were very positive:
- “Generally better speech understanding.”
- “Hear more clearly what the other passengers on the bus are talking about.”
- “I hear better at work (as a photographer).”
- “Other people tell me that I hear better; I also feel it myself.”
In summary, with the FreeFocus system, the typical user spends at least 70% of the time in Surround mode. Our focus on making listening as easy as possible with the Ponto 3 has led us to improve the most frequent listening situations, resulting in 15% better speech understanding for patients.
Fitting with Genie Medical 2016.1
The recommended fitting flow for all Ponto devices is as shown in Figure 9. First, detect the sound processor. Next, select the type of fitting (indicate whether it's single sided deafness or a Softband/headband fitting). Then, we recommend measuring the feedback limit, and lastly, to measure the BC in-situ. Note that we have changed the order. We now recommend to measure the feedback limit before measuring BC in-situ, simply to make sure that if we fit very big losses, then we can utilize the gain available in the device for the specific patient’s feedback limits. This procedure can be used for all Ponto devices. Hereafter, you can give out the Oticon Medical Streamer right from the box; you don't need to enter the serial number or do anything in Genie Medical. The Oticon Medical Streamer works with all Ponto 3 and Ponto Plus devices.
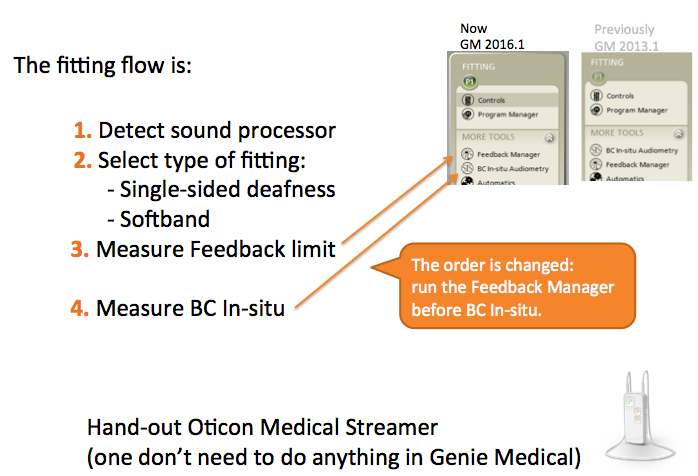
Figure 9. Recommended fitting flow with Genie Medical.
During a fitting, right when you put the device on the patient, we have a default feedback limit in the software, as indicated in Figure 10. You can also see the max gain in Figure 10.
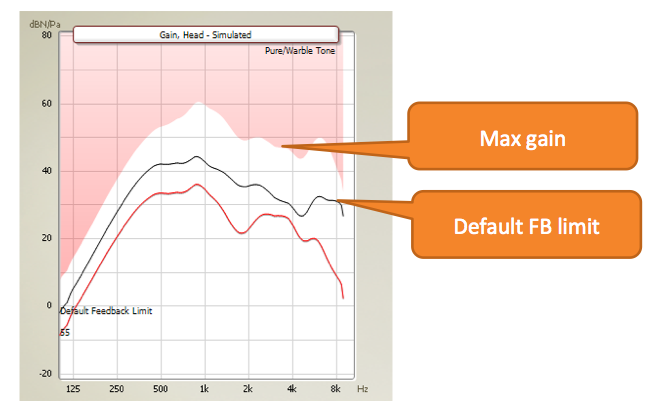
Figure 10. Default feedback limit and max gain.
The measured feedback limit will most often be at the default limit, or just above. In Figure 11, the default feedback limit is shown in the far-right graph. To the left are two examples of measured feedback limit. You can see that the measured feedback limit is almost on top of the default feedback limit, or a little above. If you measure a feedback limit that is below the default feedback limit, then it is very likely that you can decrease the risk of feedback, thereby increasing the measured feedback limit, by putting in a longer abutment. If your feedback limit is below the default, then, look at the abutment. It might be that the skin is up around the abutment, or that the device is almost touching the skin, causing the feedback limit to be very low. Changing to a longer abutment would mean that you measure a higher feedback limit. As a comparison, it would be the equivalent of making a tighter ear mold to minimize feedback in a BTE traditional hearing aid fitting.
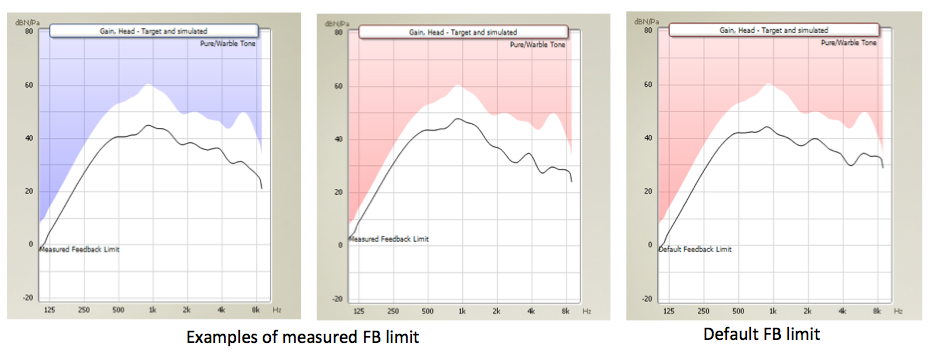
Figure 11. Measured feedback limit on abutment with Ponto 3 SuperPower.
When you measure feedback limits for devices fitted on abutment, you will typically see that the feedback limiter will determine the amount of gain that can be utilized, and not necessarily the maximum gain. There might still be some gain left above the feedback limit (Figure 12). If it turns out that the feedback limiter is limiting the gain, then you might consider manually increasing the feedback limit. You can do that in the Feedback Manager in Genie Medical. Also, you want to make sure that the Dynamic Feedback Cancellation is at maximum.
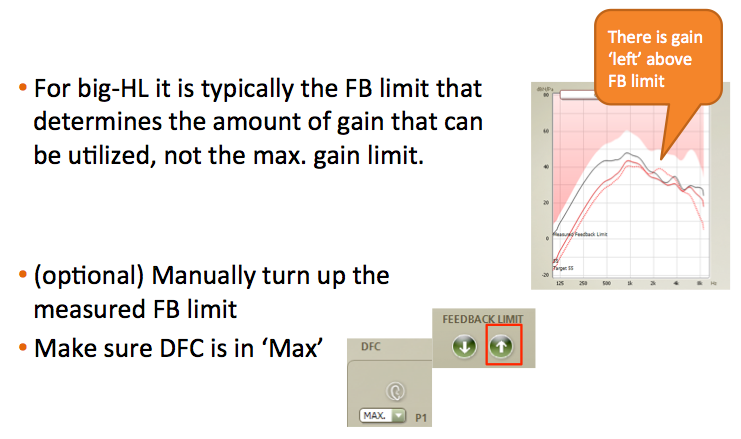
Figure 12. Measured feedback limit on abutment.
In Figure 13, you can see examples of measured feedback limits across Ponto devices. When you measure feedback limits in SuperPower and Power devices, you will roughly see that it's on par, typically because feedback is determined by physics. It might appear as if feedback limit in SuperPower is lower, but it isn't; it's because the maximum gain in the device is higher, as compared to what it is in a Power device.
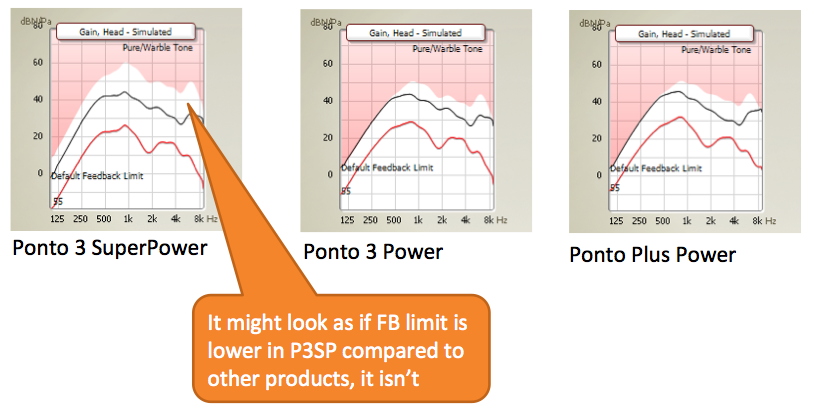
Figure 13. Measured FB limit across Ponto devices. Default and measured feedback limits are roughly the same across Ponto devices.
You may ask, “When I measure the feedback limit, will it ever be almost all the way up to the maximum gain available in the SuperPower device?” Yes, it will. In Figure 14, we show an example of a Softband fitting, where the measured feedback limit is almost all the way up to the maximum gain, and almost all the gain available in the device can be utilized. In this case, the patient can turn up the volume control a maximum of 10 dB.
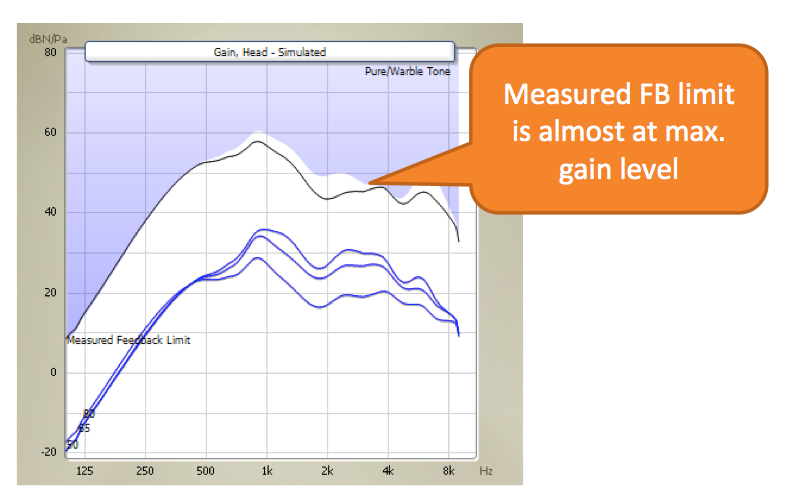
Figure 14. Softband fitting feedback limit. Feedback limit can be all the way up to max gain in a softband fitting.
Patient Reactions and Counseling
When patients with a larger mixed loss are fitted with a SuperPower device, they will typically say things like, "It sounds more calm; the sound is more pleasant; it sounds softer.” Comments that you might not expect when you fit a SuperPower device.
If we work with SSD patients, they might notice that there is no longer as much difference to the sound coming into their normal ear. This is because there is a better loudness match between the sound coming into the device, due to the larger dynamic range in the device when we use the SuperPower with a higher maximum force output.
Patients with larger mixed hearing losses, why do they report that it sounds more calm, or that it sounds softer? First of all, we have to bear in mind that patients' reactions are always related to their previous experience. You need to consider what device they used prior to testing the Ponto 3 SuperPower device.
When using a product with a higher maximum force output, a larger proportion of the dynamics in the environment and speech are reproduced without being limited by the product's maximum force output. Figure 15 shows an example of a patient fitted with Ponto 3 device. The black line represents an input of 70 dB SPL. We can see that for 70 dB SPL and any input louder, the output of the device doesn't change. The device is in saturation for an input level of 70 dB SPL. When the device goes into saturation, that will cause distortion. As an analogy, you can compare it to turning up the volume on a little radio. The sound will be distorted. It might sound loud, but it doesn't sound clear. The same happens when devices go into saturation; it causes distortion, and it sounds loud.
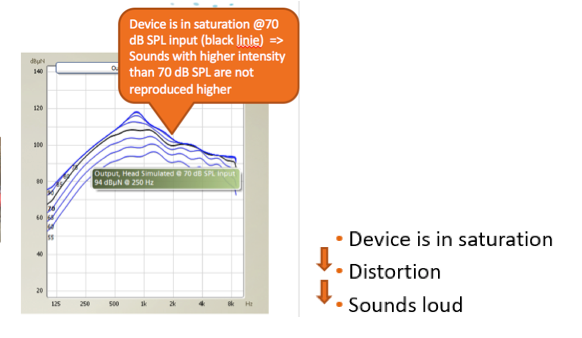
Figure 15. Ponto 3 device in saturation.
Figure 16 represents the same patient fitted with the Ponto 3 SuperPower device. Looking again at the black line, we can see that there is still room to increase the output. If we put in 75 dB SPL, or 80 dB SPL, the output is increasing. The device is less often in saturation. There are less distortion, and therefore, the device sounds quieter, or more calm. This is an explanation as to why patients have these reactions with SuperPower. In a way, it's natural; it's a consequence simply of being able to perceive more sounds without distortion. Some patients might feel a little concerned that it doesn't sound as loud as it usually does; especially those with more significant mixed hearing losses.
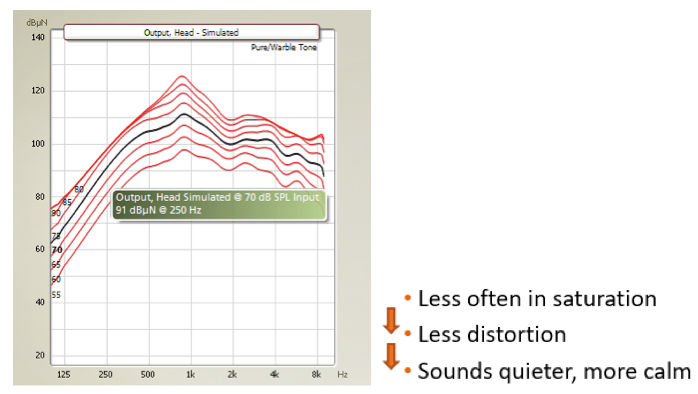
Figure 16. Ponto 3 SuperPower fitted to the same patient as in figure 16. Ponto 3 SuperPower is less often in saturation and distortion.
A recent study was conducted at Radboud University in Holland (Bosman et al., 2017). They had a total of twenty participants, nineteen of which used a Ponto Pro Power, and one who used a Baha Intenso. They were all fitted with the SuperPower device. In Figure 17, you can see that the average bone conduction threshold was 30 dB HL down to 40-45 dB HL.
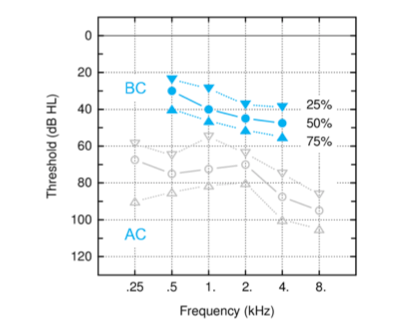
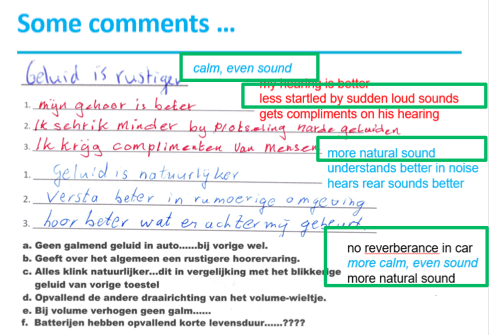
Figure 17. Left: Preliminary results of pure tone audiometry (n=20); Right: Patient comments. From P3SP test Nijmegen (Bosman et al., 2017).
Afterwards, all the patients preferred the Ponto 3 SuperPower device. Some of them commented that it sounded more calm and more natural with the SuperPower. Other participants remarked that they could understand better in noise, they could hear sounds better from the rear, and that they did not experience any reverberation while driving in a car. One participant in the study went into the street wearing the device, and an ambulance passed by. He came back and was surprised how much quieter, and more pleasant it sounded. This can be attributed to lower levels of distortion with the SuperPower device.
Patient Counseling
Patients often have the perception that loudness and speech understanding are tied together; that it needs to sound very loud in order for them to understand speech. However, we can counsel patients that loudness and speech understanding are two separate things. With the SuperPower device, it might not necessarily sound as loud, but the speech will be easier to understand, and the sound will be clearer. We would recommend that you also demonstrate this to patients, in addition to counseling them. The demonstration will make a bigger impact on them than just talking about it.
DSL-BC Fitting Rationale
For the first time, the well-known DSL fitting rationale is now tailor-made for BAHS (Hodgetts & Scollie, 2016). It is called DSL-BC. It was developed by Susan Scollie from University of Western Ontario, and Bill Hodgetts from University of Alberta. The rationale builds upon the same principle as the DSL for traditional hearing aids: to map the natural dynamic range to the patient's dynamic range (residual auditory area). The input parameters to the rationale include the patient's BC in-situ hearing threshold, and the maximum force output of the device. This, coupled with information about real head to coupler differences (RHCD) that is known for each device (already in Genie Medical). Using this formula, they prescribe the amplification to fall within the auditory dynamic range. The DSL rationale comes in an adult and a pediatric version. The pediatric version provides a little bit more amplification, such as is known for traditional hearing aids, as children are developing their language.
Compared to NAL-NL1 (the rationale that we've had in the devices since the introduction in 2009), the DSL-BC rationale provides:
- Less low frequency amplification
- Less amplification for conductive hearing loss
- Some higher amplification (and compression ratio) for larger mixed HL
The DSL-BC rationale is available in all Ponto devices on the market. If you have patients who are already fitted with a Ponto device, you can have them fitted with DSL. It is also possible to have DSL in one program, and the NAL rationale in another program. In the preference menu, you can choose which rationale should be the default.
FLogram
I'll briefly go over some of the new features in Genie Medical. The FLogram is a new way to look at a fitting. The FLogram is to bone anchored devices, what SPLogram is to air conduction devices. The FLogram shows everything in the graph and the output of the device in dBµN. The gray line in the FLogram (Figure 18) is the normal hearing reference, the Reference Equivalent Threshold Force Level (RETFL-dBC). It is measured with direct sound transmission via an abutment. The FLogram is true for and reflects a fitting on abutment; it doesn't reflect a fitting on Softband. The RETFL is equivalent to a 0 dB HL, as known from the audiogram view.
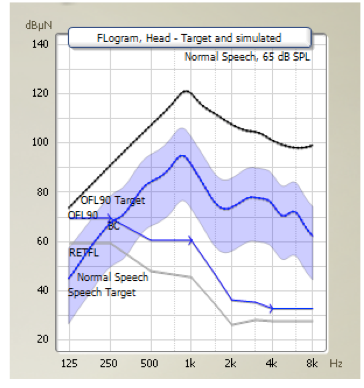
Figure 18. FLogram, with Normal hearing reference, RETFL-dBC (gray line), BC hearing loss (lower blue line), aided speech spectrum (shared blue area) and Output for 90 dB SPL input (OFL90) (black line).
An FLogram makes it very easy to judge audibility, because you can see and compare the patient's BC hearing threshold as measured with BC In-situ, the output force level for 90 dB SPL input (OFL90), and the aided normal speech spectrum. Anything above the gray line (Figure 19) is audible, while the part of the speech under the gray line on the far left, in the very low frequency, isn't audible.
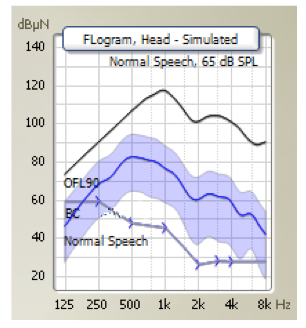
Figure 19. FLogram in Genie Medical.
If you start using the FLogram, you have to get used to the fact that the hearing threshold level will look very different than what you're used to, because it's all shown relative to the RETFL. In this example (Figure 20), we see that at 4 kHz, there is a 30 dB HL hearing loss; we have that reflected that the difference between the gray line (RETFL-dBC) and the blue line (the hearing loss) is 30 dB.
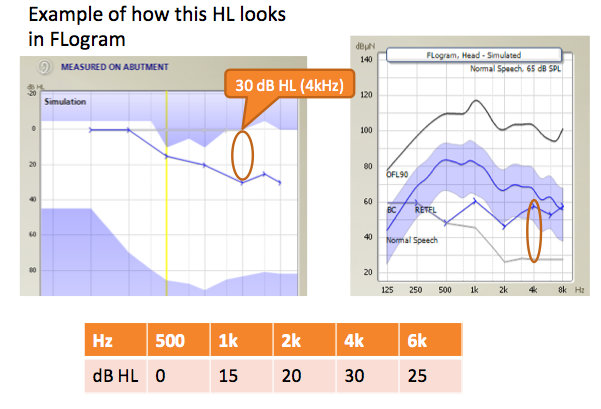
Figure 20. Example of how a mild sloping hearing loss looks in FLogram.
With theFLogram, we now have three views/graphs in Genie Medical: An Output view, an FLogram view, and a Gain view (Figure 21). Each view has its own advantages. The Output is useful to judge saturation in devices, FLogram is useful for judging audibility, and the Gain view is useful for seeing the feedback limit, and how much the patient can increase the volume.
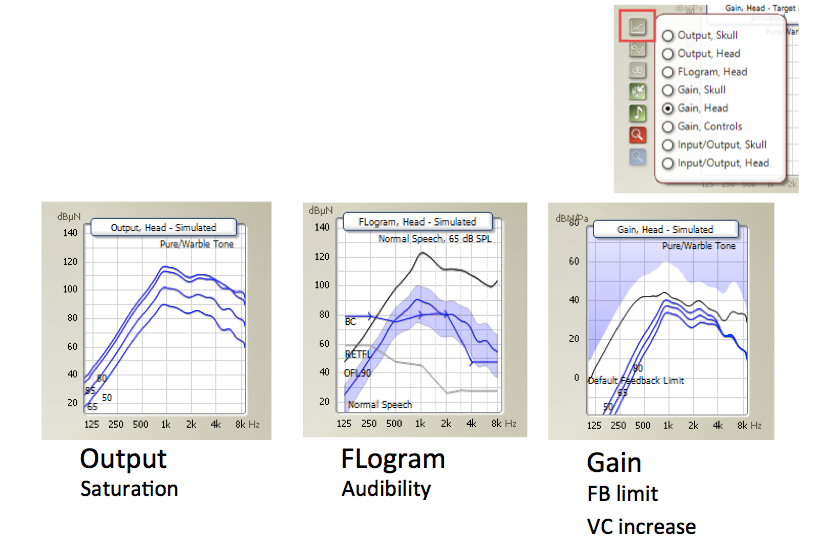
Figure 21. Three views in Genie Medical.
Summary and Conclusion
To summarize, although we have a SuperPower device, the maximum force output does not exceed patient's loudness discomfort level. All patients can benefit from a higher maximum force output in Ponto 3; especially, those who need additional gain because they have a hearing loss in the cochlea, a mixed hearing loss, SSD, or if they wear a Softband. The FreeFocus directionality, with the new Speech Focused mode, increases speech intelligibility by 15%. When patients are fitted with Ponto 3 SuperPower, they would typically describe the sound as being more calm and natural, because the device is less into saturation. The DSL-BC rationale is available in all Ponto devices. Finally, FLogram is useful for judging audibility.
With theFLogram, we now havethree views / graphs in Genie Medical: An Output view, an FLogram view, and a Gain view (Figure 22). Each view has its own advantages. The Output is useful to judge saturation in devices, FLogram is useful for judging audibility, and the Gain view is useful for seeing the feedback limit, and how much the patient can increase the volume.
Questions and Answers
For pediatric patients, can you discuss again the possibility of the Ponto 3 SuperPower being too loud? Is there a risk of over-amplification with Ponto SuperPower?
If we have a child with bilateral atresia, for example, that child has never listened to loud sounds. The first step when fitting children, is to obtain the parents' acceptance for us to provide amplification to their child. That buy-in is important, that's step number one. You can fit the SuperPower right from the start; there is no risk of over-amplification. However, if the parents would only accept a smaller device, then I would start using the Ponto 3 device. The child will initially begin to learn language through direct interaction with their parents (at 1 -2 years old). As they get older, they begin to communicate with and learn language from other children. When they enter school, they are exposed to environments that are much more dynamic. At the latest at that point in time, I would recommend fitting the child with SuperPower.
References
Bosman, A.J., Mylanus, E.A.M., Hol, M.K.S., & Snik, A.F.M. (2016) Wireless and acoustic hearing with bone-anchored hearing devices. International Journal of Audiology, 55(7), 419-424. DOI: 10.1080/14992027.2016.1177209
Bosman, A., Hol, M., Snik, A.F.M., & Mylanus, E.A. (2014, May). Evaluating Oticon Medical Ponto Plus and Ponto Pro Sound Processor. AudiologyOnline, Article 12616. Retrieved from: https://www.audiologyonline.com
Bosman et al. (2017, February). Data presented at Oticon Medical Scientific meeting, Denmark.
Hodgetts, W.E., & Scollie, S.D. (2017). DSL prescriptive targets for bone conduction devices: adaptation and comparison to clinical fittings. International Journal of Audiology, DOI: 10.1080/14992027.2017.1302605
Lunner, T., Rudner, M., Rosenbom, T., Ågren, J. & Ng, E.H.N. (2016). Using speech recall in hearing aid fitting and outcome evaluation under ecological test conditions. Ear & Hearing, 37, 145S- 154S.
Oticon Medical. (2016). FreeFocus feature test report. Oticon Medical report no 34425-00. Somerset, NJ: Oticon.
Wagener, K., Josvassen, J.L., & Ardenkjær, R. (2003). Design, optimization and evaluation of a Danish sentence test in noise. International Journal of Audiology, 42, 10-17.
Citation
Rosenbom, T. (2017, June). Ponto 3 SuperPower, new treatment option to BAHS patients. AudiologyOnline, Article 20376. Retrieved from www.audiologyonline.com

