Learning Outcomes
- Describe why own voice is an issue for hearing aid wearers.
- Describe how Signia Nx Own Voice Processing (OVP) works.
- Describe the validation study conducted with OVP.
Introduction
You twenty-to-thirty-something readers probably grew up hearing your own voice from some recording—telephone messages, home movies, tape recordings, and other devices. And today, hearing your own voice via a recording probably sounds pretty normal to you, or at least tolerable. It was only a generation or two ago, however, when hearing one’s own recorded voice was a novel experience. It would immediately illicit emotional cries of “That’s not me!” “I don’t sound like that, do I?” or “I can’t stand to listen to myself.” The point here is that our perception of our own voice is very important and personal, and that’s what we talk about in this article.
Why does our own voice sound so abnormal when we hear it from a recording? There are a couple reasons. First, the overall spectrum of the sound reaching the microphone of the recording device is different from that which reaches our eardrums when we talk. The latter is influenced by head shadow and diffraction, ear canal resonance and pinna effects. Probably the biggest factor, however, which determines our perceptions of our own voice is the contribution that is transmitted via bone conduction. The vocal folds set the skull into vibration and this reaches the cochlea. The bone-conducted component tends to make our voice sound lower and richer, which of course is missing from the recorded sample.
Like people with normal hearing, people with hearing loss also rely heavily on the bone-conducted signal of their own voice to determine what is “natural.” Perhaps even more so than people with normal hearing, as in many cases, the high frequency components of their speech normally heard by air conduction are no longer audible.
Hearing Aids and Own-Voice Satisfaction
Hearing aids usually make the issue worse. In the MarkeTrak VIII survey, Kochkin (2010) addressed own-voice satisfaction for individuals using hearing aids, and found that only 58% of respondents gave the rating of “satisfied” or “very satisfied” for the sound of their own voice. Recently, Hoydal (2017) reported own-voice satisfaction based on a survey of nearly 400 hearing aid users; 78% had used their hearing aids for more than two years. The majority had mild-moderate loss, and although not stated in the report, we suspect that many, if not most had open fittings. In this study, only 41% were satisfied with the sound of their own voice. Similar findings were reported by Powers, Froehlich, Branda and Weber (2018), who found that for new hearing aids users fitted to the NAL-NL2, only 34% were satisfied with how their own voice sounded while using the hearing aids.
Consider that the goal of most all hearing aid fittings is to optimize speech understanding. This involves programming gain and output so that it maximizes benefit when listening to a communication partner. Since most hearing aid users have a significant hearing loss in the higher frequencies, we normally see the greatest gain in this region, especially for soft inputs. While this works well for speech understanding, this is not the optimum programming to make the patient’s own voice sound natural. Moreover, their own voice often is louder, and head shadow and diffraction changes the spectrum.
Own Voice Processing (OVP)
What is needed is a hearing aid that instantaneously changes gain and output whenever the person talks, which is now available with the Signia Nx, using an algorithm termed Own Voice Processing (OVP). When OVP is activated, the wearer’s own voice is detected and processed separately, while external sounds remain unaffected. Whenever the patient is speaking, through bilateral data sharing, processing and analysis, the hearing aids identify this signal, and apply a dedicated setting, which differs from when only external sounds are present. This acoustic analysis and own-voice initialization only requires a few seconds of live speech from the user while wearing the hearing aids. During this initial training, the hearing aids “scan” the acoustic path of their own placement, relative to the location of the sound source. The patient’s head shape and mouth placement relative to the hearing aids is part of the sculpturing to create an accurate detection. Based on this analysis, the hearing aids will then be able to detect when sound (speech) is coming from the patient, versus the surroundings, even if speech is coming from a conversation partner directly in the front. This detection is independent of vocal effort or the specific utterances of the user. See Hoydal (2017) for further detail regarding the OVP analysis.
Research Evidence for OVP
There is research evidence to show that when using OVP, hearing aid users actually perceive their voice to sound more natural. A study on this topic recently was completed at the University of Northern Colorado, as part of a larger study on OVP (Powers, Froehlich, Branda and Weber, 2018). The participants (n=21; 12 males and 9 females, mean age 67 years) were all new hearing aid users and had bilateral symmetrical downward-sloping hearing losses. The hearing aids used were the Signia Pure 7Nx, and they were fitted bilaterally. Following the initial fitting of the hearing aids, each participant did the OVP training that we described earlier. The Signia Connexx software led through the training procedure and indicated when the own-voice initialization was complete, which typically required 10 seconds or so of vocalization from the patient. Once the OVP initialization was finished, the participants read familiar nursery rhymes aloud, and compared four different settings of the OVP: off, mild, moderate and strong. After several short samples at all four conditions, each participant selected the setting that they believed resulted in their own voice sounding “most natural.” The setting selected was subsequently used for all OVP “on” vs. “off” comparisons for each participant.
Ratings of the naturalness of their own voice were accomplished using a 13-point, 1-7 scale: 1=Very Unnatural, 4=Neutral, and 7=Very Natural. Ratings were made on a worksheet in front of the participants, allowing them to see the rating for the previous condition. The OVP-On vs. OVP-Off was randomized and the participants were blinded to the processing. For all own-voice ratings of naturalness, the participants read aloud passages of familiar nursery rhymes.
Fitting Conditions
There were several fitting conditions. The study looked at the benefit for OVP for NAL-NL2 fittings versus the Signia proprietary fitting, Nx-fit. It also examined how the openness of the ear-canal coupling influenced OVP benefit by conducting naturalness ratings for closed and open fittings. Finally, ratings of naturalness for Signia (with OVP) were compared to the ratings for two competitive products without this feature.
Findings
The NAL-NL2 fittings using a closed ear dome were all verified with probe-microphone measures. Therefore, there was a confirmed (within 2-3 dB) NAL-NL2 fitting in the ear canal. Individuals rated the “naturalness” of their own voice with OVP-On versus OVP-Off. Figure 1 is a summary of the distribution of the ratings for all the participants for the two different conditions. There is agreement from previous studies, showing that a large percent of hearing aid users do not believe their own voice sounds natural when using hearing aids—note the OVP-Off data. With OVP-Off, only 29% gave a rating higher than “neutral,” and importantly, 42% rated the naturalness of their voice negatively.
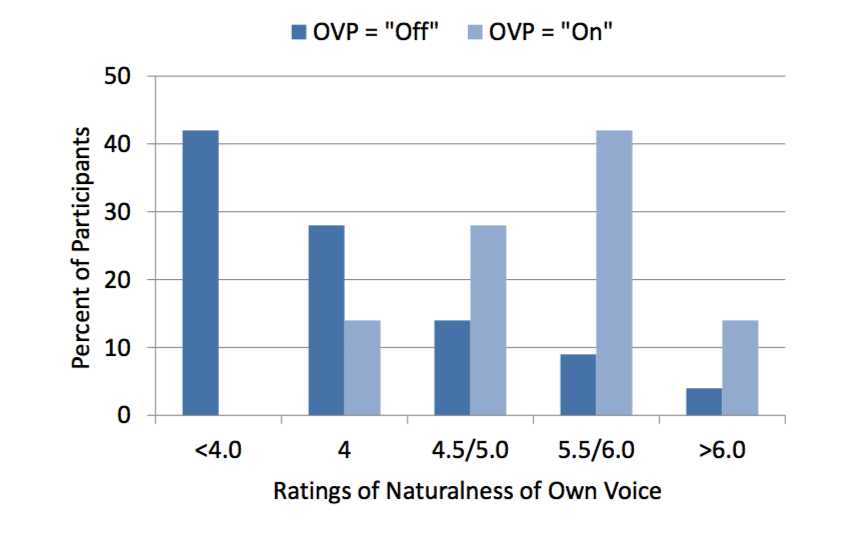
Figure 1. Individual distribution of own-voice naturalness ratings for OVP-Off vs. OVP-On. The participants were fitted using closed ear tips with hearing aids programmed to the NAL-NL2 prescriptive algorithm. The naturalness of their own voice was rated on a 13-point scale (1=Very Unnatural, 4=Neutral, and 7=Very Natural).
A very different picture emerges when OVP is activated (Figure 1). Observe that now, there are no negative ratings for naturalness, and only 14% gave the rating of “neutral.” The remaining 86% had positive ratings (above 4.0) with the majority at the 5.5 or 6.0 category; a desired rating of “natural.” No participant had a lower rating for OVP-On compared to OVP-Off, and only two participants did not give a higher rating for OVP-On; one of these gave a #7 rating for OVP-Off, and therefore a higher rating for OVP-On was not possible given the limits of the scale.
There was a significant group advantage for OVP-On. The mean values for the two conditions are shown in Figure 2 (error bars represent 95th confidence interval). As shown, on average the naturalness rating went from below 4.0 (“neutral”) to 5.5. Statistical analysis, using two-tailed t-test, revealed this difference was significant (p<.001).
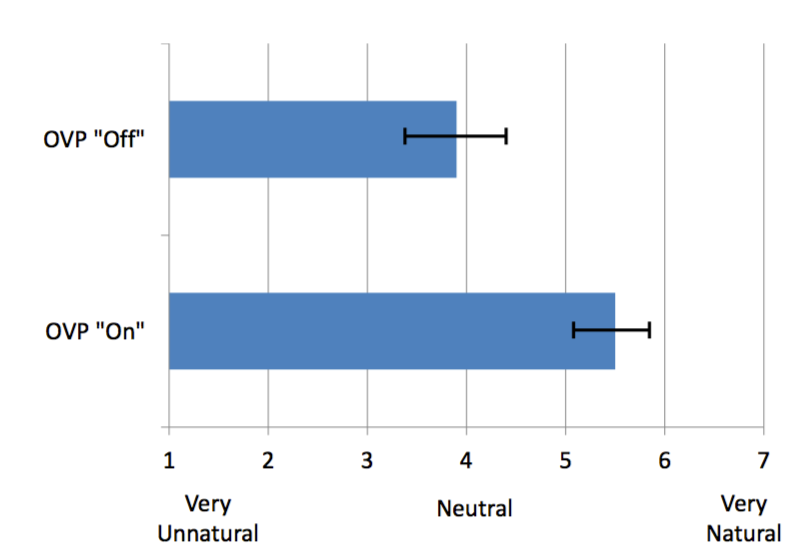
Figure 2. Mean own-voice naturalness ratings for OVP-Off vs. OVP-On (error bars represent 95th confidence intervals). The participants were fitted using closed ear tips with hearing aids programmed to the NAL-NL2 prescriptive algorithm. The naturalness of their own voice was rated on a 13-point scale (1=Very Unnatural, 4=Neutral, and 7=Very Natural).
OVP and Signia Nx-fit. A second area of interest was to study the effects of OVP when Signal Nx-fit is used. Nx-fit is a prescriptive algorithm developed to optimize the performance of Signia instruments. One of the considerations in the development was to create a pleasant listening impression, including the sound of one’s own voice. It is not surprising, therefore, that participants judged their own voice to sound more natural with this fitting, than when they were fitted with the NAL-NL2. But, just the same, there were even better ratings for this fitting when OVP was activated (Figure 3).
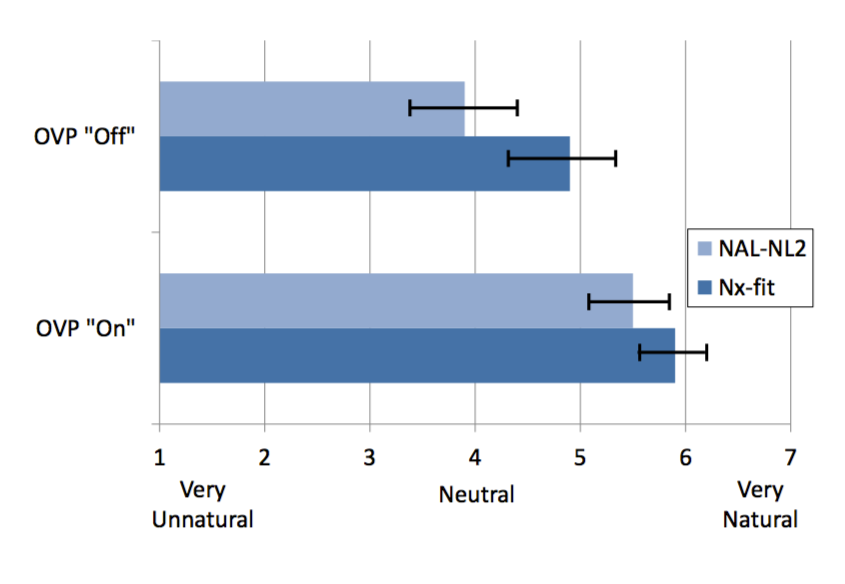
Figure 3. Mean own-voice naturalness ratings for OVP-Off vs. OVP-On for NAL-NL2 and Nx-fit (error bars represent 95th confidence intervals). The participants were fitted using closed ear tips with hearing aids programmed to the Signia Nx-fit (NAL-NL2 own-voice natural ratings also included for comparison). The naturalness of their own voice was rated on a 13-point scale (1=Very Unnatural, 4=Neutral, and 7=Very Natural).
Observe that the mean rating for Nx-fit with OVP-Off was 4.9, 1.0 better than when the NAL-NL2 was employed (p<.001). There is also a mean 1.0 improvement in the naturalness rating for Nx-fit when OVP was activated (p<.001). With OVP activated there was a 0.4 advantage for the Nx-fit compared to the NAL-NL2, although this was not significant (p>.05). This suggests that clinicians can obtain the same high level of own-voice naturalness with closed fittings regardless if they use the NAL-NL2 or the Nx-fit prescriptive algorithm.
OVP and Open Fittings
It might be tempting to think that patients don’t have issues with their own voice when fitted open, but this isn’t true. While they are less likely to report “hollowness,” they often find their amplified voice to be sharp, shrill, hissy, etc. To examine OVP with open fittings, all participants were fitted with the Signia open tips, with the hearing aids programmed to Nx-fit. The ratings for naturalness were obtained in the same manner as before, for both OVP-Off and OVP-On. The mean ratings are shown in Figure 4. As expected, with OVP-Off, the mean ratings were higher than when the same participants were fitted with a closed eartip. But, there still was a significant advantage for OVP (mean rating increasing from 5.5 to 6.1; p<.001). If we view the individual distribution with OVP-Off, only 48% gave a rating of 6.0 (“Sounds Natural”) or better, whereas with OVP-On, 86% gave a rating of 6.0 or better, with no participant giving a rating below 4.0 (“Neutral”).
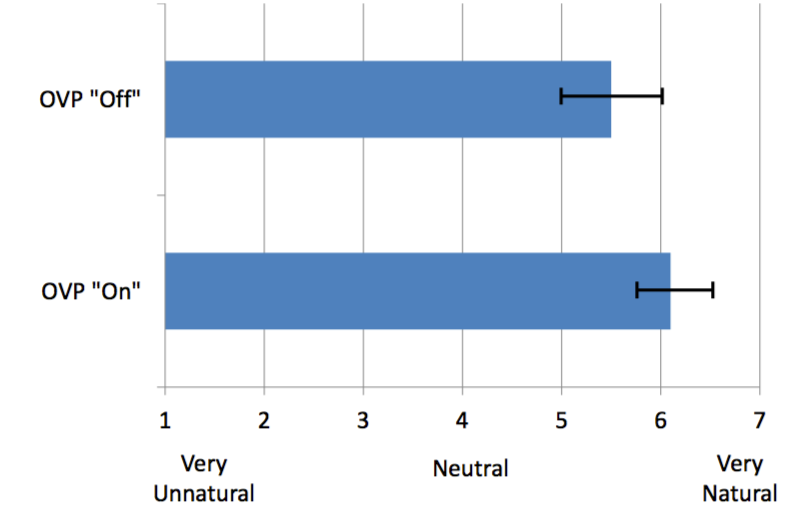
Figure 4. Mean own-voice naturalness ratings for OVP-Off vs. OVP-On (error bars represent 95th confidence intervals). The participants were fitted using open ear tips with hearing aids programmed to the Signia Nx-fit. The naturalness of their own voice was rated on a 13-point scale (1=Very Unnatural, 4=Neutral, and 7=Very Natural).
OVP versus Competitors
In addition to examing OVP-On versus OVP-Off, OVP processing was compared to competitive products from other manufacturers. The premier mini-BTE RIC products were selected from two leading manufacturers, and they were fitted to NAL-NL2 (verified with probe-mic measures), using the closed ear tip recommended by each manufacturer. To ensure that the fittings were similar in their tightness of fit, a real ear occluded response (REOR) was conducted for all fittings, including the Signia NAL-NL2 fittings discussed earlier. There was no significant difference at any frequency for the mean REOGs for the three different manufacturers, suggesting that the different ear tips produced fittings that were equally closed.
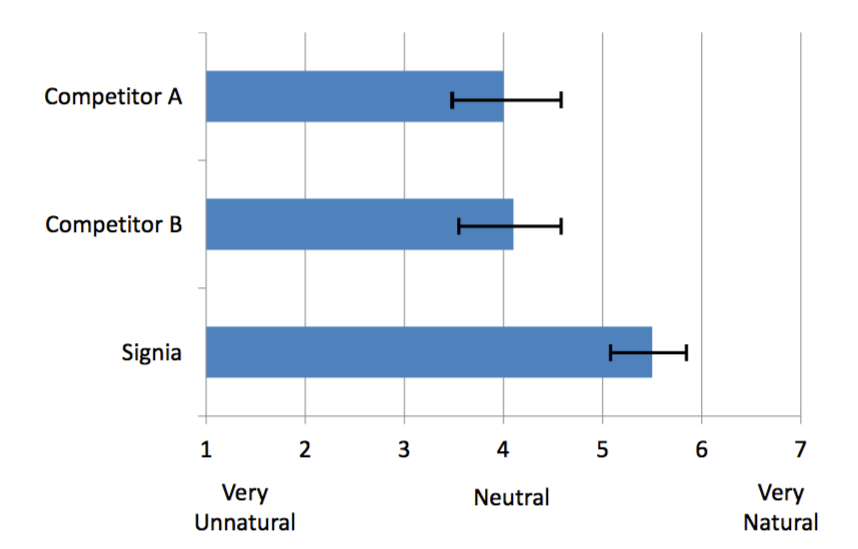
Figure 5. Mean own-voice naturalness ratings for Signia and two competitive products (error bars represent 95th confidence intervals). Participants were fitted with closed ear tips and the hearing aids were programmed to NAL-NL2. The naturalness of their own voice was rated on a 13-point scale (1=Very Unnatural, 4=Neutral, and 7=Very Natural).
The mean ratings for own-voice naturalness for the two competitive products are shown in Figure 5. Also included for comparison are the data from Signia, previously displayed in Figure 2. As shown, mean naturalness ratings were very similar for Competitor A and B, with a large advantage noted for the Signia product. Statistical analysis of these data reveal higher own-voice ratings for the NAL-NL2 closed condition for Signia compared to both Competitors A and B (p<.001). A naturalness rating of “Somewhat Natural” or higher was obtained from 95% of participants when fitted with Signia, but only 32% for Competitor A and 37% for Competitor B.
Advantage for Signia for Open Fittings
For the voice-naturalness ratings for an open fitting, each manufacturer’s proprietary fitting algorithm was used, as well as their recommended open tips. These results were then compared to the previous testing with Signia (see Figure 4), and the mean findings for all three brands are shown in Figure 6.
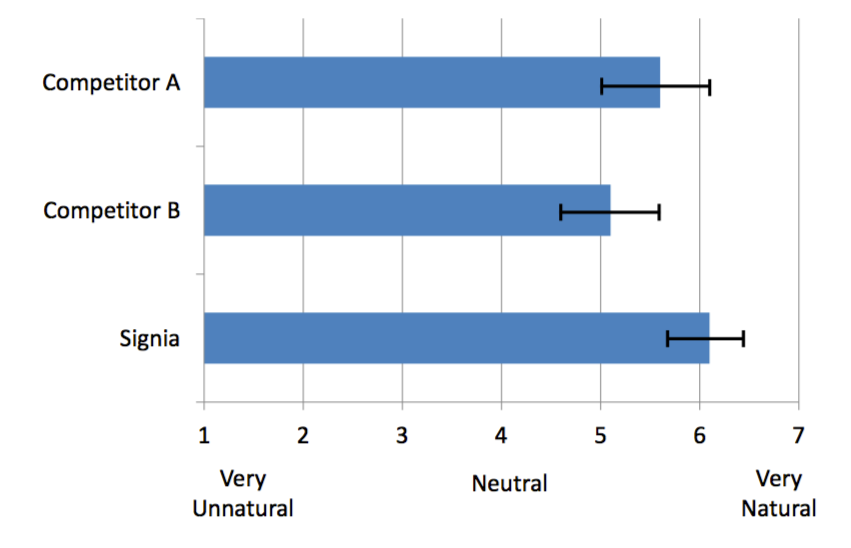
Figure 6. Mean own-voice naturalness ratings for Signia and two competitive products (error bars represent 95th confidence intervals). Participants were fitted with open ear tips and the hearing aids were programmed to each manufacturer’s proprietary algorithm. The naturalness of their own voice was rated on a 13-point scale (1=Very Unnatural, 4=Neutral, and 7=Very Natural).
For the open fitting condition, there was a significant advantage for the Signia product (p<.05 for Competitor A; p<.001 for Competitor B). What is also an important finding from a clinical standpoint, is that the Signia Nx-fit closed fitting (Naturalness rating of 5.9; see Figure 3), is equal to the open fitting of Competitor A, and superior to the open fitting of Competitor B (p<.05).
The open-fitting results were examined on an individual basis (Figure 6). For this comparison, participants were identified who, when fitted with each manufacturer’s proprietary fitting, had an own-voice naturalness rating of either “Natural” or “Very Natural.” Importantly, the Signia data shown are for both a closed fitting and open fitting; the data for the competitive products was obtained with an open fitting. A large difference in individual rating of naturalness was observed—71% for Signia closed, and 86% for Signia open, compared to 58% and 37% for the two competitors.
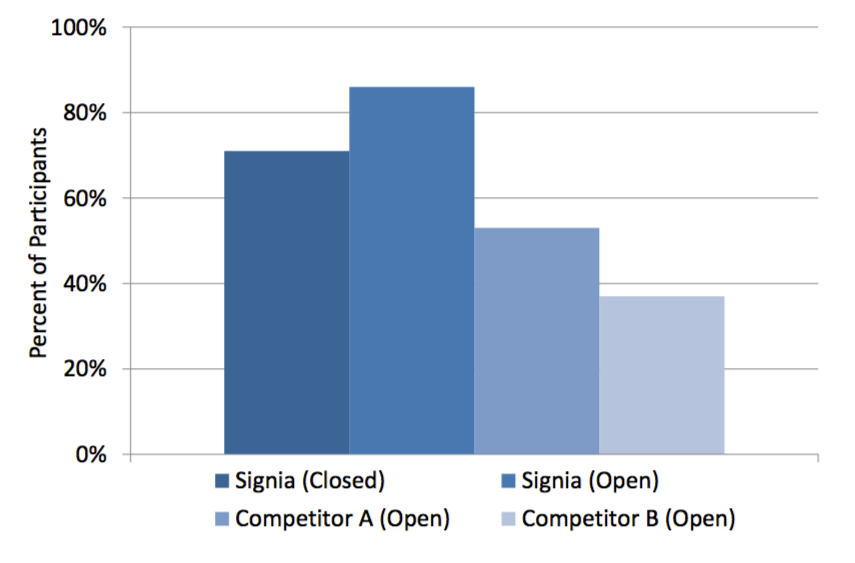
Figure 7. Percent of participants that rated their own-voice naturalness #6 (“Natural”) or higher. The naturalness of their own voice was rated on a 13-point scale (1=Very Unnatural, 4=Neutral, and 7=Very Natural). Results are shown for Signia (both closed and open fittings) and for two competitive products with open fittings. The hearing aids were programmed to each manufacturer’s proprietary fitting algorithm.
OVP and the Occlusion Effect
There are two issues that could cause own-voice problems regarding own-voice naturalness: the amplified signal from the hearing aid (which is what we have been discussing) and what is commonly called the occlusion effect. What causes the occlusion effect? As reviewed by Mueller, Ricketts and Bentler (2017) the process goes like this:
- When we talk, certain sounds, especially vowels, reach 120 to 130 dB SPL, or more in the back of the throat.
- The high intensity sounds travel via the mandible (bone conduction) to the condyle, which is adjacent to the ear canal.
- This bone-conducted signal (typically below 750 Hz) then becomes an air-conducted signal by vibrating the cartilaginous portion of the ear canal (in general, the lateral two-thirds).
- In normal situations (unaided), this low-frequency energy escapes out of the open ear canal and doesn’t contribute significantly to our perception of our own voice.
- If the lateral portion of the ear canal is plugged with a hearing aid or earmold, this signal cannot escape, and the resulting trapped energy in the residual ear canal volume is reflected back to the eardrum and transmitted to the cochlea in the typical air conducted manner.
- These sounds will then change the perception of our own voice and can also increase the sounds of chewing (particularly crunchy foods), and even vascular noise and breathing. Because the occlusion effect affects mostly the vowels of speech, and some vowels more than others (e.g., there is little effect for the /ah/), not only does the voice sound louder, but also unusual (booming, hollow, echo, etc).
By following the pathway just described, which is what causes the occlusion effect, it is clear that the process is not related to the signal going through the hearing aid or to amplification provided by the hearing aid. This is why OVP will have little impact on the occlusion effect.
How does the clinician differentiate between own voice issues due to the occlusion effect vs. problems related to hearing aid amplification? As mentioned earlier, the occlusion effect is unrelated to the amplified signal. This means that the occlusion effect will be the same with the hearing turned on as when the aid is muted. This is an easy way to quickly check the origin of the own-voice issue. It works well to have the patient read aloud a passage containing the vowels that are the most impacted, such as the /ee/, with the hearing aid turned “on” vs. “off.” Mueller, Ricketts and Bentler (2017) offer this suggestion: “Through three cheese trees three free fleas flew.”
If it is determined that the issue truly is the occlusion effect (voice is annoying when hearing aid is turned off), then the treatment is venting—allowing the energy to escape. The occlusion effect typically has its maximum in the 200 to 500 Hz area, which fortunately are frequencies that respond reasonably well to venting. In fact, many “closed” fittings have enough slit leak to accomplish at least some venting for these frequencies. Recall that earlier, REOGs for the closed domes of three different manufacturers was discussed. In general, the mean REOGs for each manufacturer (42 fittings) were around -2 dB for 250 Hz and -1 dB for 500 Hz, suggesting venting was occurring for these lower frequencies. With a custom-made tight fitting traditional earmold, with no venting, it’s common to see REOGs of -10 to -15 dB.
A Few Words about Ampclusion
The term “ampclusion” is sometimes used in articles about the hearing aid occlusion effect. Unfortunately, the term has led to some misunderstanding regarding the treatment of the occlusion effect. The term was coined by Steve Painton in a 1993 article. According to Painton (1993), ampclusion is “the combination of occlusion and low-frequency amplification that results in the ‘hollowness’ or ‘head in the barrel’ complaints.” As reported by Mueller, Ricketts and Bentler (2017), the “combined” effects, however, usually are not the major clinical issue. Consider, that if the occlusion effect and the hearing aid output were at the same frequency range and the same intensity, the combined effect, would be no more than 3 dB (and that is only if the two signals were equal). It is possible that there could be an occlusion effect problem at 200 Hz, and too much gain at 500 Hz, but usually the problem is one or the other. If the issue really is ampclusion, however, then OVP will provide benefit, and it very well could be that once the amplified signal is improved, the remaining occlusion effect will no longer be annoying.
OVP as a Fitting Solution For Nearly All Patients
OVP is appropriate for both open and closed fittings, and for different fitting rationales. In many cases, in particular open fittings, when asked about how their own voice sounds, patients will often say “okay.” In the past, this may have been a satisfactory answer. The current study shows that even when the patient says “okay,” implementing OVP might change that response to "excellent". It seems reasonable, therefore, to give the option of OVP to essentially all patients. While most of this work has been limited to individuals with mild-to-moderate hearing loss, it is unusual for a patient to rate OVP-On as sounding less natural than OVP-Off.
Conclusion
An added bonus of OVP is that high own-voice naturalness ratings can be obtained with a closed fitting. Open fittings are popular, but there are some downsides. The effectiveness of noise reduction will be reduced in the low frequencies—the very region where it is most desired, as the noise has a direct pathway to the ear drum. Likewise, the directivity index of directional hearing aids is reduced significantly. What might provide a 5-6 SNR advantage with a closed earmold, easily could be reduced to 3-4 dB with an open fitting. And of course, even with the best feedback cancellation system, an open fitting might not allow for the desired gain in the high frequencies due to feedback issues. The data presented here clearly show that with OVP, it is possible to maintain own-voice naturalness with a closed fitting, to the extent that ratings for Signia OVP with a closed fitting are equal to or better than competitive products with an open fitting. This allows for taking advantage of all the other feature benefits that provide the needed audibility and noise reduction for the patient.
References
Høydal E. (2017). A new own voice processing system for optimizing communication. Hearing Review, 24(11), 20-22.
Kochkin, S. (2010). MarkeTrak VIII: Consumer satisfaction with hearing aids is slowly increasing. The Hearing Journal, 63(1), 19-20.
Mueller, H., Ricketts, T., & Bentler, R. (2017). Speech mapping and probe microphone measurements. Plural Publishing Incorporated.
Painton, S. (1993). Objective measure of low frequency amplification reduction in canal hearing aids with adaptive circuitry. Journal of the American Academy of Audiology, 4(3),152-156.
Powers, T., Froehlich, M., Branda, E., & Weber, J. (2018). Clinical study shows significant benefit of own voice processing. Hearing Review. 25(2), 30-34.
Citation
Froehlich, M., Powers, T., Branda, E., & Weber, J. (2018, April). Perception of own voice wearing hearing aids: why “natural” is the new normal. AudiologyOnline, Article 22822. Retrieved from www.audiologyonline.com




