Case 1 - Fluctuating hearing loss
The first topic I would like to discuss is fluctuating hearing loss. Fluctuating hearing loss is certainly familiar to audiologists, especially to those audiologists who work with children, and it is a particularly important issue. Brain development occurs through auditory input. If the child is not getting good, consistent auditory signals due to fluctuating hearing loss, then that child's auditory brain development will be affected;things like language and speech development, speech perception, and other skills may be negatively impacted.
What are the issues in managing children with fluctuating hearing loss?
The first and maybe the most difficult issue is in determining that hearing is indeed fluctuating. When we're working with young children, they're not in a position to tell us that something is happening with their hearing. Parents of children who are just beginning to develop speech and language often are not sure if the child's lack of attention to auditory stimuli is just simply a lack of attention, if it is a hearing issue, or if it is caused by something else.
We need to carefully monitor children who have middle ear disease to determine if their hearing is fluctuating. Exactly how often to monitor will vary depending on the child. Children who have a history of middle ear disease several times during the winter should be monitored every 6-8 weeks during the winter and spring when middle ear disease is most common. One of the first things we need to do is educate other professionals who care for these child, particularly the pediatricians and the ENTs who may not always consider a child's hearing when there are repeated ear infections. We need to inform the families and the school personnel about the negative effects of fluctuating hearing loss. Children with middle ear disease may have decreased hearing for as much as six weeks as a result of one episode of middle ear disease. If you consider a child who has three ear infections in a year, which is not unusual, that means there may be as many as 18 weeks in a year in which that child is not hearing normally. This is a not a minor issue and something that all audiologists need to pay careful attention to.
We also need be aggressive in monitoring fluctuations in hearing. If we have a child either with
hearing loss or without hearing loss that has middle ear disease and it is suspected that there may be a fluctuation we need to get that child in for testing. It is not unusual for a parent to call to schedule a test and be told that the next opening on our schedule is not for three or four weeks. As clinicians we need to make adjustments to get that child in quickly - within 2-3 days. This may mean educating our office staff or those responsible for scheduling about how to recognize which appointments may need to be squeezed in.
One question to consider is, "How much fluctuation matters?". Which brings a follow-up question, "Is mild hearing loss really mild, especially in children?". I, for one, would like a different term other than "mild" that is more descriptive of the actual difficulties that children with mild hearing loss encounter. The term mild implies that the hearing loss is not significant. A 15 dB drop in hearing may not be significant to an adult, but it is very significant to a person who is trying to learn language or to manage in school. If a child's normal hearing thresholds are at 15 dB HL and there is a drop of another 15 dB due to fluctuating hearing loss, then that puts that child's thresholds at 30 dB HL, in the mild hearing loss range. At 30 dB, soft speech is essentially inaudible or unintelligible. That child is only hearing conversation at normal listening levels of 50 dB. For listening to soft speech and to speech in competing noise that child is at a very significant disadvantage. Therefore, any hearing loss (thresholds poorer than 15 dB HL) for an infant or child is significant and should be very carefully monitored. I would like to share some data from a study I conducted that was published as part of a chapter I wrote in the textbook Evidence-Based Otitis Media, by Richard M. Rosenfeld and Charles D. Bluestone, editors (1999). This study looked at word recognition of 12 children with bilateral middle ear effusion in four different listening conditions. The listening conditions were: normal conversational level in quiet;normal conversational level in noise;soft conversational level in quiet;soft conversational level in noise. The normal conversational level was 50 dB HL, the soft conversational level was 35 dB HL, and the noise conditions had a signal-to-noise ratio (SNR) of + 5 dB (four talker babble). The word lists used were appropriate for the age of the child (i.e., NU Chips for children 3-6 years;WIPI for children 4-6 years;PBK for children in kindergarten and 1st grade;NU 6 for 2nd grade and above). Even with middle ear effusion, these children all had normal hearing, meaning that their thresholds were 15 dB HL or better. But with middle ear effusion, their speech perception was negatively affected, as can be seen in Table 1.
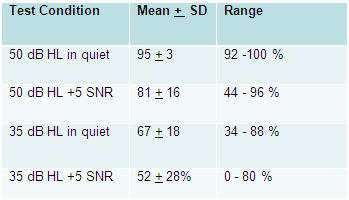
Table 1. Word recognition for 12 children with bilateral middle ear effusion and normal hearing. Adapted from Madell (1999).
At the normal conversational level in quiet all the children did very well;scores ranged from 92 - 100% with a mean of 95%. If you stopped the testing here, you would have the impression that these children are doing fine. However, when noise is added to the equation and when the speech becomes softer, the outcomes are very different. At the normal conversational level in noise, the mean was 81% and there was a very wide range of performance with some children's scores dropping as low as 44%. At soft conversational level even in quiet, all the children were struggling;scores ranged from 34% - 88%. And at the soft conversational level in noise, the average was 52%, with a range from 0% to 80%. One thing that should be very evident by this data is that if you are only testing speech recognition in quiet at normal conversational levels, you cannot predict how children will perform in other situations or if they are struggling in conditions that are more typically-occurring in the real world. If we really want to determine whether or not a child is struggling or having difficulty, we need to conduct our testing in conditions that the child will actually encounter, including soft speech and in competing noise. Testing in quiet and at normal conversational levels alone is not sufficient.
Five of these children then had pressure equalization (PE) tubes put in and were subjects in a follow-up study (Rosenfeld, Madell & McMahon, 1996). They were tested after getting PE tubes in the same conditions that were tested pre-operatively in the previous study: 50 dB HL in quiet;50 dB HL in noise with a + 5 dB SNR;35 dB HL in quiet;35 dB HL in noise with a + 5 dB SNR. Their results can be seen in Table 2.

Table 2. Impact of PE tubes on word recognition. Adapted from Rosenfeld, Madell & McMahon, (1996).
As can be seen from the data, post-operatively all the children did well in every condition, with postoperative scores across conditions ranging from 92% - 100%.
Regarding management, I discussed the importance of educating parents and caregivers, physicians and teachers about fluctuating hearing loss, as well as the need for aggressive monitoring when a fluctuating hearing loss is suspected.
For children with hearing loss who use amplification, we need to manage the technology when there is fluctuating hearing loss. If a child has frequent changes in hearing, we need to determine if the current hearing aid settings are appropriate during a period of fluctuation. If not, we can create a special program in the hearing aids, for example, with more gain and output, as appropriate, for the decreased hearing. Then the parent can switch into that program during a fluctuation.
A FM system is an option for children who may have normal hearing, except during an episode of otitis media. When decreased hearing occurs, the FM system can be available for use at home and in school so that we know that child has sufficient auditory access and can hear during a fluctuation. Ideally, the school system or clinic will have FM loaners for use with children during episodes of middle ear disease. Classroom modifications may also be useful during periods when hearing is compromised.
Lastly, we need to encourage aggressive medical management to reduce or prevent middle ear disease and the accompanying fluctuating hearing loss that can occur.
Case 2 - Testing infants
This is one of my favorite topics. One of my goals is to encourage more clinical audiologists who work with babies to do behavioral testing, and that is what we will be discussing here.
It is established protocol to perform an auditory brainstem response (ABR) test for infants who fail a hearing screening or when a hearing loss is suspected. After an ABR is done and a hearing loss is confirmed, we have to determine if the parents are ready to accept the ABR results as a confirmation of hearing loss and if they are ready to move on with amplification. Often times they are not. We also have to determine, as clinicians, if we have adequate information from ABR results to proceed with fitting and programming hearing aids on that infant. ABR is not a direct measure of hearing but rather a measure of brainstem functioning. We know fairly well how it correlates to hearing, although 10 to 15 decibels can make a significant difference in the fitting of amplification. In my experience, most audiologists are not comfortable with fitting hearing aids based only on ABR results and will proceed cautiously and conservatively in terms of programming gain, output and other amplification characteristics. This approach may not always provide the child with the optimal acoustic input and sufficient auditory access. Yet another challenge arises when it comes to monitoring the child's progress with amplification;it is not practical to perform routine aided ABRs to monitor hearing aid benefit.
For these reasons, we turn to behavioral observation audiometry (BOA). BOA is consistent with the early identification philosophy. Parents can observe the infant during testing, hear the stimuli and see their infant's responses. This establishes for parents a better sense of what their child is hearing and the importance of moving forward with amplification. This facilitates making early treatment recommendations to parents as it may help to establish a level of concern in the parents and enhance follow-up. BOA provides a confirmation of the electrophysiological test results. Further, it provides information about the child's ability to attend to auditory stimulation, which is not available from electrophysiological testing. Maybe, the most useful thing BOA can help with is monitoring responses with technology. With BOA we can determine if the child is receiving sufficient benefit from hearing aids.
BOA, when performed appropriately, is very accurate. The method that I recommend involves observing changes in sucking. BOA is a very reliable technique when the behavior you are observing is changes in sucking. The infant can either nurse at the breast, suck from a bottle or use a pacifier. It is important to use only sucking behaviors to obtain thresholds for BOA. Other behaviors, such as changes in respiration or limb movement, are not threshold responses and therefore should not be counted as responses for the purposes of BOA. To learn more about this method, refer to the book that Carol Flexer and I wrote entitled Pediatric Audiology: Diagnosis, Technology and Management (Madell & Flexer, 2008). The book includes a DVD-ROM that features straightforward directions on how to perform BOA as well as videos of various pediatric behavioral assessments with audio commentary. I also presented a course on BOA on AudiologyOnline entitled Behavioral Evaluation of Hearing In Babies - Yes, You Can that outlines BOA and also includes videos of this procedure being performed on infants where you can observe the responses. It is available for viewing as a recorded course in the AudiologyOnline course library.
Table 3 shows you the thresholds of a child who was tested using BOA at age 6 weeks, and later was subsequently tested using VRA at age 8 months and play audiometry at age two-and-a-half years. This child is a sibling of a child with hearing loss. As can be seen by the table, this child's responses are essentially the same using BOA, VRA and play.

Table 3. Thresholds for the same child obtained via BOA at age six weeks, VRA at age six months and play audiometry at age 2.5 years. Adapted from Madell & Flexer (2008).
Table 4 shows the thresholds of another child obtained by BOA at age five months, VRA at age 16 months, and play audiometry at 2.5 years.

Table 4. Thresholds for the same child obtained via BOA at age 5 months, VRA at 16 months and play audiometry at 2.5 years. Adapted from Madell & Flexer (2008).
Again, you'll see all thresholds obtained via BOA are consistent with those obtained using VRA and play audiometry.
These are just a few examples of the reliability of BOA results using a sucking response. To develop skill and comfort with conducting BOA, try it on every infant you see either before or after the ABR test. Eventually, use it to confirm your electrophysiological test results, to monitor hearing over time and to monitor hearing aid benefit over time. If you see infants and young children in your practice, BOA is a necessary and invaluable clinical procedure. It works, it is reliable and it will make all the difference in your management of children with hearing loss.
Case 3 - Identifying Problems with Technology
In the best case scenario, we are identifying children with hearing loss through newborn hearing screening and timely follow-up testing, we are fitting them with appropriate amplification at approximately four weeks of age, and we are comfortable with reliable methods of verifying and validating the fitting.
Now our job is to monitor the technology to ensure it is continuing to work for that child over time. We need to ensure that the technology is doing what it needs to do when it needs to do it. More specifically, we need to ensure that the child can hear soft speech. Soft speech is about 35 dB HL. We need to be sure that a child's aided thresholds are above 35 dB HL so that soft speech is audible. If a child's thresholds are at 40 dB HL, that child is not hearing soft speech at all. If aided thresholds are at 15 dB HL, soft speech is coming in at 20 dB SL and that is probably going to be okay. We also need to know how a child hears in the presence of competing noise. We know that understanding speech in noise is a significant problem for people with hearing loss, and that noise in classrooms is at about + 5 SNR. So it is critical that we test in noise so we know how a child is likely to perform in the classroom.
Goals of assistive technology
The goal of assistive technology is first to reduce sensory deprivation and second to provide auditory access that is sufficient for auditory learning. This means maximizing the child's use of residual hearing and laying the foundation for auditory academic learning so that the child can use hearing in the classroom the same way his typically-hearing peers do. Assistive technology needs to facilitate socialization so that the child can use hearing to communicate with those around her in play situations. Assistive technology needs to provide safety so that the child knows things are happening around him, and it needs to be comfortable. It needs to facilitate information access, extended learning and incidental learning.
Children learn a great deal by overhearing conversations around them. That is incidental learning. We all know of experiences where a child repeats something she has heard and we wonder how she knew that or where she picked it up.
That is a critical part of learning. Children with hearing impairment need to be able to do that. If they are not hearing well, then they are going to be missing out on an enormous amount of incidental learning. Children need to have sufficient hearing in order to be able to overhear and take advantage of incidental learning.
How do we know if a child's technology meets these goals? Does real-ear verification or cochlear implant mapping provide enough information? It is my philosophy that it does not tell us enough. By performing real-ear testing, we can determine how much sound is reaching the eardrum. That is an important first step in fitting amplification but it is not enough. We also need to know what the child perceives from the amplification we are providing. That means we need to verify in a test booth using aided thresholds with the child's technology- whether it be hearing aids, cochlear implants, FM system or a combination.
If the child is in school we also need to verify how the child is performing in the classroom. We need to know what the child is hearing in the classroom and in what situations he may be having difficulty. An audiologist or teacher of the deaf can conduct some testing in the classroom to help determine how the child is hearing. The child's speech perception at close distances and at far distances can be measured in the classroom to see how the child is performing. Parent/teacher questionnaires can also help us to figure out what is happening. The SIFTER (available from the Educational Audiology Association), CHILD (Anderson & Smaldino, 2000), LIFE (Anderson & Smaldino, 1996) or COW (Williams, 2005) are all useful questionnaires.
The first thing that is involved in determining how a child is doing with his technology is measuring if a child is hearing enough high frequency sounds. Hearing very well through 1000 Hz or through 2000 Hz and then dropping off to 35 dB HL in the higher frequencies is not sufficient. That means that the child is not hearing /s/, /sh/, /f/ and other high frequency consonants, and is therefore missing pluralization, possession, and all kinds of grammatical markers which affect language, reading and academic development. In addition to verifying adequate high frequency amplification, the perception of soft speech needs to be verified. For the child to hear soft speech at 35 dB HL, thresholds need to be well above that level. Next, we need to see if the child is hearing well enough with each ear individually. This is an important point. If testing is only conducted binaurally, it may be that the child is getting more from one device or the other. The ears should be matched whenever possible, and it is not okay if one is hearing much better than the other. In some cases, there is nothing that we can do about it. However, unless we test each ear separately with the technology we don't know that. It is our goal to have children be binaural listeners, not just bilateral listeners;we want them to use both ears and to be hearing the same in each, if possible. This is critical for localization and for understanding speech and in noise.
Therefore, an evaluation should at least consist of word recognition testing with amplification in the eight conditions listed in Table 5. The test will differ depending on the child's language abilities. Children who have a receptive vocabulary below 3 years should be tested with the ESP (Moog & Geers, 1990). Children age 3-6 years should be tested with the NU Chips (Elliott & Katz, 1980);4-6 years, WIPI (Ross & Lerman, 1971);kindergarten level, PBK. For children at 2nd grade level and above can be tested using adult word lists such as the NU 6.

Table 5. Recommended test conditions for word recognition testing with amplification.
Testing in these conditions, at a minimum, should let us know if we need to modify the technology to improve performance.
Let's look at a case where aided testing was performed and the management decisions that were made as a result. Figure 3 is the audiogram of child L.B. who has a moderate to severe hearing loss.

Figure 1. Aided thresholds for child L.B. with moderate to severe hearing loss.
If you look at the speech banana in Figure 1 you will notice that I have a dark green line at the top of the speech banana. I would like to suggest that instead of having a speech banana we have a speech string bean, because our goal is to have the child hear at the top of the banana. If you hear at the top of the banana you hear 90% of what is said. If you hear at the bottom of the banana you hear 10% of what is said. We sometimes give the impression to parents that if the child hears anywhere within the speech banana it is sufficient, but that is not case. 10% clearly is not sufficient. 90%, at the top of the speech banana, must be our goal.
L.B.'s aided thresholds fall between 30 - 40 dB HL, which means that this child is going to hear normal conversational level but is not going to hear soft conversation at all. This is not sufficient. The speech perception testing for this child can be found in Table 6.

Table 6. Speech perception test results for child L.B.
L.B.'s speech perception in the left ear is much poorer than the speech perception in the right ear. Look at the binaural score. The poorer left ear is negatively impacting binaural speech perception. This child could not perform for soft speech or for speech in noise because the basic information was not loud enough.

Figure 2. L.B.'s aided results, with new hearing aids.

Table 7. L.B.'s speech perception scores, with new hearing aids.
L.B.'s hearing aids were at maximum, with no reserve gain that could be increased, so she was fitted with new hearing aids that provided more amplification. Figure 2 shows her aided results after receiving new hearing aids. Her improved aided results were not the result of any learning period, as they were obtained two days after the results with her old hearing aids. Table 7 shows her speech perception scores with her new hearing aids. Her speech perception with her old technology was 72% in the right ear, 52% in the left ear. With new hearing aids, her scores were 92% in both ears and 100% binaurally. As you can see, at soft conversational level her score was 92%, and at normal conversational level in competing noise, 80% with the increased amplification that the new hearing aids provided.
Case 4 - Identifying the need for more therapy
As audiologists, we sometimes focus just on hearing aids and don't think of ourselves as being responsible for monitoring other aspects of a child's auditory performance. We test auditory performance to determine if there is a need for a change in technology such as a changing in hearing aid settings or moving from a hearing aid to CI or adding an FM. We also should be testing to monitor auditory development.
We are in a very unique position. Teachers in the classroom and parents are seeing their children every day. The speech language pathologist or auditory verbal therapist is maybe seeing a child twice per week. All of these people are seeing the child on a very regular basis, but audiologists are not. As children adapt to the hearing aids and seem to be doing well, the time between testing can be extended. This is variable for each child. We see children when they are first fit with amplification maybe every 4 6 weeks, eventually every three months and then twice a year or annually as the children get older. So we are in a good position to monitor progress. If a child is not making progress we may be able to see that before other professionals or the parents see it.
Speech perception should improve over time. We need to determine if the child has sufficient speech perception to manage in a classroom setting. That includes hearing conversation in the classroom from other children, hearing the teacher, and also hearing in the lunchroom and at recess. Also, we need to know what a child can understand with and without an FM system, and to determine what other assistance may be needed - a notetaker, teacher of the deaf, computer-assisted real-time transcription (CART), or maybe some auditory based speech-language therapy.
Let's look at a couple of audiograms here.

Figure 3. Child with severe hearing loss, good aided thresholds but poor speech perception.
Figure 3 shows an audiogram of a child with severe hearing loss who has aided thresholds at 20 - 25 dB HL. From my point of view this is good hearing as this child has a lot of auditory access. But look at the speech perception scores - 28% in one ear and 24% in the other using a speech perception test that is appropriate for the child's vocabulary. This child came for cochlear implant evaluation because she was performing poorly.
A cochlear implant is not going to provide this child with more auditory access. This child is doing very poorly despite good auditory access, so the first thing I would look at in managing this child is if the child needs some additional auditory therapy by a clinician who is trained to do auditory-based therapy. This is usually a speech-language pathologist or teacher of the hearing impaired but may be an audiologist. The person doing the therapy needs to be specifically trained to provide auditory-based therapy. If this child had some auditory-based therapy we might improve the child's speech perception before we moved on to other recommendations.
Table 8 shows unaided thresholds of another child with a severe hearing loss, and aided thresholds in the 30 - 40 dB range in both ears.

Table 8. Child with severe hearing loss, and aided thresholds in the 30 - 40 dB HL range. Adapted from Madell & Flexer (2008).
These thresholds are not sufficient for hearing and understanding soft speech. In terms of management, the first I would look at is monitoring the technology. Note that the speech perception is much better for the right ear than the left ear. It may be that the slight difference in the aided thresholds explains the difference in speech perception since the right ear aided thresholds are 5 - 10 dB better than the left. Or, it may be that the child needs more help working on the left ear alone, with auditory therapy.
Case 5 - Is it time for a cochlear implant?
This case involves making a decision about whether a child hears well enough with hearing aids, or if it is time to move to a cochlear implant (CI). When a child uses hearing aids, we need to ensure that they are providing enough hearing for language learning, academic learning, and socialization. In these cases especially, it is important to collaborate closely with the child's teachers and therapists.
If the child is not hearing well enough with hearing aids, we need to look at changing the hearing aids or the hearing aid settings to make a difference. We want to know if the child is receiving adequate high frequency information and if the child is FM dependent. If the child can only function with hearing aids when using an FM system, this may be a child that needs more assistance.
We've talked about auditory access in earlier cases. The question arises, how good is good enough? How much auditory access a child needs does not differ depending on the technology or the degree of hearing loss. Does a child with hearing aids need to hear less than a child with normal hearing? I think the answer to that is no. Children with hearing aids and children with CIs need to hear the same as children with normal hearing. Our goal in fitting technology is to see that children with hearing loss hear as much as those with normal hearing can. While we cannot make it perfect and we cannot give them normal hearing, our goal is to have them as close to normal hearing as possible.

Figure 4. Test results of child with profound loss and very poor speech perception scores. Aided thresholds were obtained with child's hearing aids.
Figure 4 shows test results from a child with a profound hearing loss and very poor speech perception with hearing aids, 12% in one ear and 8% in the other. You can see he is hearing from the middle of the speech banana to outside the speech banana with his hearing aids. He's doing very poorly. This child received an implant by the age of 16 which is late by today's standards but this was some years ago. Using his CI his binaural speech perception scores went from 16% with his hearing aids to 64%. With hearing aids, we had been unable to test soft speech and speech in noise. While I don't think this child is doing well with his technology, using a CI we were able to obtain 56% for soft speech and 64% for normal conversation in noise which significant improvement from his performance with hearing aids. In this case, the child has a profound hearing loss with best possible hearing aid fitting and was not getting enough benefit. It was clear that this child needed to move to a CI.
Figure 5 shows results from a child with severe hearing loss. The child has good auditory access - although he's not hearing at 15 dB HL, he is hearing with his technology at 20 - 25 dB HL.

Figure 5. Audiogram and speech perception testing results from child with severe hearing loss.
His speech perception is fair to good with 76% in the right ear, 74% in the left ear and 88% binaurally. With the FM, it's 96%. His scores for soft speech and speech in noise are not good but he is doing well with the FM in those conditions. Therefore, this is a child I would continue to closely monitor but would not necessarily see as an immediate need for a CI.
Figure 6 shows test results from another child with a severe hearing loss.

Figure 6. Child with severe hearing loss. Aided thresholds in high frequencies with hearing aids not providing enough auditory access, therefore poor speech perception scores.
For some reason we cannot get this child's aided thresholds better than 35 - 40 dB HL in the high frequencies. This child is missing an enormous amount of information. This is a child who is not getting enough hearing with hearing aids no matter what we've tried, therefore, this is a child we moved to a CI.
Figure 8 shows test results from a child with a severe bordering on profound hearing loss who is not doing well with hearing aids.

Figure 7. Child with severe-profound hearing loss whose aided thresholds with hearing aids do not provide sufficient auditory access.
He received a CI on the right side and you can see aided results in Figure 8.

Figure 8. Aided thresholds and speech perception results using hearing aid left ear, and cochlear implant right ear for same child as Figure 10.
With his CI, his aided thresholds are 20 dB HL across frequencies. You can see that the CI made a very significant difference for him. He has since gotten a second CI.
Figure 9 shows the audiogram of a 6-year-old child who would be considered off-label for CI use.

Figure 9. Results from 6-year-old girl who would be considered off-label for CI use due to good low frequency hearing thresholds.
She has good low frequency hearing and very poor hearing starting at 750 Hz and beyond. We were able to obtain an SRT but could not do a PBK test with this child due to the severity of the loss. This is considered off-label CI use due to the good low frequency hearing thresholds, although it is not usable low frequency hearing. Most surgeons will use hearing preservation protocols for surgery in this type of hearing loss. This child is very bright and has language but she needs to be able to see your face in order to understand you.
She was implanted in her right ear. Results with the implant can be seen in Figure 10.

Figure 10. Results from child in Figure 12 following cochlear implantation on the right ear.
Within a period of a few months, her speech perception was 80% in the right ear with the implant. It was 7% in the left ear with the hearing aid, 88% binaurally, 54% for soft speech and 48% for normal conversation in noise.
Case 6 - Does this child need FM?
Classrooms are very noisy. The SNR in classrooms is between -7 and + 5. Listening all day is hard work, and even more challenging when the signal is not clear such as when it is too soft or when noise is present. Figure 11 shows test results from a child who does very well at normal conversation but when you test him for soft conversation and speech in noise he's clearly struggling. When we added the FM we made a significant difference for normal conversation, and not enough of a difference for speech in noise, which I cannot explain. This was a child who ended up having significant auditory therapy in order to learn to function better in a noisy situation.

Figure 11. Unaided, aided and aided + FM results for 8 year old child.
The next example brings up the question, "What is good enough?" Table 9 shows the test results from a child who is having significant difficulty with hearing aids alone;when an FM system is added he makes a significant improvement.

Table 9. Speech perception scores with hearing aids, and with hearing aids + FM.
If we test this child and we show him these kinds of test results, it's easy to convince even a third or fourth grader who initially tells you that they are doing fine without an FM system to use one. I show them the scores and ask them, "Is 68% good on a math test?" and they know it isn't. Then they're willing to bargain about when they're going to wear an FM system.
Summary
Thank you for your attention and I hope you found these cases interesting. You'll note a recurring theme or goal in management for all the cases we discussed today. That goal is ensuring children have sufficient auditory access in a variety of situations including for normal and soft conversation, in quiet and in competing noise, in the classroom and in real-world situations. Sufficient is defined as as close to normal as possible in each ear individually and binaurally. As audiologists identifying and managing children with hearing impairment, our testing procedures, technology choices, recommendations and advocacy all need to be aligned with that goal.
References
Anderson K.L., & Smaldino, J.J. (1996). Listening inventory for education: An efficacy tool (LIFE). Available from www.karenandersonconsulting.com
Anderson, K. L. & Smaldino, J.J. (2000). CHILD: Children's Home Inventory for Listening Difficulties. Available from www.edaud.org and www.phonak.com
Elliott, L.L., & Katz, D. (1980). Development of a new children's test of speech descrimination (Technical Manual). St. Louis, MO: Auditec.
Madell, J. R. (1999). Impact of otitis media on auditory function. In, R. M. Rosenfeld and C.D. Bluestone (Eds), Evidence-based otitis media (pp. 337 - 351). Hamilton, Ontario, Canada: B.C. Decker, Inc.
Madell, J.R. & Flexer, C.A. (2008). Pediatric audiology: Diagnosis, technology, and management. NY: Thieme.
Moog, J.S, & Geers, A.E. (1990). Early speech perception (ESP) test. St. Louis, Mo: Central Institute for the Deaf.
Rosenfeld, R.M., Madell, J.R. & McMahon, A. (1996). Auditory function in normal hearing children with middle ear effusion. In D.J. Lim, C.D. Bluestone, M. Casselbrant, J.O. Klein & P.L. Ogra (Eds.), Recent advances in otitis media: Proceedings of the 6th International Symposium (pp. 354-356). Hamilton, ON, Canada: B.C. Decker Inc.
Ross, M. & Lerman, J. (1971). Word intelligibility by picture identification. Pittsburgh: Stanwix House.
Williams, C. (2005) The children's outcome worksheets - An outcome measure focusing on children's needs (ages 4-12). News from Oticon, January 2005. Available from www.oticon.com

