
Editor’s Note: This text course is an edited transcript of a live webinar. Download supplemental course materials.
Kimi Moller: Today I will talk about The Mild Misnomer: Diverse Needs for Mild Hearing Impairment. The “mild misnomer” suggests little or no experience with impairment or handicap for the people with mild hearing loss. This is misleading, because a mild hearing loss can have significant consequences for some people in their everyday lives.
Learning Objectives
I will start today with definition of mild hearing loss and discuss how many people are wearing hearing aids. Then I will go through expectation management for this group, followed by mild hearing loss solutions, including hearing aids and accessories. I will end with some common fitting errors for these hearing losses.
Mild Hearing Loss
Audiologists have different ways of defining mild hearing loss. How do you define a mild hearing loss? Common answers include 26 to 40 dB, difficulty hearing in noise, normal low-frequencies sloping down at 2000 or 3000 Hz, and not being able to hear soft voices or sounds. The definition by Clark (1981) is exactly 26 to 40 dB. That means that fricatives are compromised most in the higher frequencies.
The prevalence of hearing loss in adults was measured by the World Health Organization in 2011, and the findings were presented in 2012. Across all the world, the highest percentage of hearing impaired people have mild hearing losses from 26 to 40 dB. This count also estimates that one-third of persons above 65 years of age have some sort of disabling hearing loss.
The majority of hearing impaired people have mild hearing losses (WHO, 2012). With that said, do you also think they are the majority of people who own hearing aids? The correct answer is no. MarkeTrak (Kochkin, 2009) and EuroTrak (Hougaard & Ruf, 2011) studied hearing aid adoption rates for four different categories of hearing loss (mild, moderate, severe, and profound). There were not enough people from the United Kingdom (U.K.) who answered the EuroTrak questionnaire to divide between severe and profound hearing loss, so those numbers are combined into one group.
The trend across these countries seems to be that a higher percentage of people engage in hearing technology as the hearing loss gets worse. Only between 6 and 14% of people with mild hearing loss across Germany, the U.K., France and the United States obtain hearing aids. The U.K. provides free hearing aids from the government, so more people with mild hearing loss are likely to give them a try, which is why they have the highest adoption rate for mild hearing loss.
Dillon and colleagues (Dillon et al., 2010) did a study where they asked people how much they wanted to get hearing aids when they went for an evaluation, from “very much” to “did not want.” They also asked them to rate how much difficulty they thought they were having when not wearing their hearing aids. The people who experienced less difficulty reported not really wanting the hearing aids. And, the more severe the hearing loss, the more people felt that they needed the hearing aids. These data may not be surprising.
Hearing Instrument Adoption
Why is it that more people with mild hearing loss do not get hearing aids? There can be many reasons, but I will cite three circumstances. First are the practical reasons. People with mild hearing loss might not even be aware that they have a hearing loss. The loss may come on gradually, and they may not have a problem in every situation. Ear pain and ear allergies may prevent people from getting a hearing aid. Manual dexterity issues in some patients might make them think they could not handle the hearing aid. It can also be the financial aspect of spending money on something that they do not feel is a big problem.
Second are all the psychological reasons, the first of which is denial. Patients may say, “It is not me who has the problem. My friends and family are mumbling.” I have also encountered people with mild hearing losses not wanting hearing aids because they are afraid they would further damage their hearing. They may also fear the outward sound of feedback. It is up to us as audiologists to educate people about the function and rehabilitative capacities of hearing aids.
Third are the social reasons. The fear of being seen as old and incompetent makes people wait as long as they can, and they tell themselves that their problem is not that bad. No matter the reasons people make for postponing or declining hearing aids, we have to take the clients’ fears and worries seriously, no matter what they are. If they come into our clinic, we have to make sure they get the right rehabilitation and set the expectations correctly.
Expectation Management
Expectation management is important, no matter which person you are fitting or counseling. But with this subset of patients, since they often experience fewer problems, expectation management is even more important. Mecklenburger & Joergensen (2009) studied how much benefit people with mild hearing loss can receive from wearing hearing aids. They used an Abbreviated Profile of Hearing Aid Benefit (APHAB) questionnaire, which contains 30 questions that are answered on a 7-point scale that corresponds to the percentage of time a patient feels it applies to the question. Initially, the questionnaire is answered without wearing hearing aids. After wearing the hearing aids for a prescribed amount of time, patients answer the same questionnaire again, not having access to their previous answers. You can then compare answers with and without the hearing aids.
They studied 85 people with mild to moderate hearing losses who were all fit with open fittings. Then they compared it to the Cox & Alexander (1995) norms, which do include users with severe hearing loss and closed fittings. The results were divided into four categories. One is ease of communication, where all questions in that group are in regard to communication with their communication partners. Another category is reverberation, or how well they do in rooms with a lot of reverberation. The third category is background noise, or how well they understand speech in background noise. The last category is aversiveness to loud sounds, or how bothered they are by loud sounds.
The 85 people that Mecklenburger and Joergensen (2009) included in their trial had fewer initial problems without the hearing aids than the normative group that included mild, moderate and severe hearing losses. That also makes the mild hearing loss group more difficult to please, as they do not experience problems in every situation; therefore, hearing aids cannot help them in every situation.
Overall, the more time that users have with hearing aids, the more their reported problems decrease. This means there is some sort of benefit. The perceived benefit of the open-fitted group with mild to moderate loss is less than the normative group, but we have to walk away with the bigger picture that even the people with mild hearing impairment do benefit from amplification.
When fitting people with mild hearing losses, we have to be more realistic in our expectations because they have fewer difficulties. We need to only fit the people who are motivated to get amplification. Those who are not yet motivated for amplification likely need to be counseled first.
Tools for Communication
Motivation is the key for positive outcomes. Some tools for counseling and determining motivation can be found on the Ida Institute’s website, www.idainstitute.com. The two that I like the most for when I encounter new clients are the line and the box.
The Line
The line only requires pen and paper if you have the client sitting in front of you. Draw a line and put 0 at one end and 10 at the other (Figure 1). Then ask the patient questions, such as, “How important do you feel that it is for you right now to improve your hearing?” The patient will put a mark somewhere on that line to indicate how motivated they are to do something about their hearing.
Figure 1. The line motivational tool.
Let’s say they mark a 3. You can start talking from that perspective. A 3 is probably not very motivated to do anything, so you should ask why that is. That can start a good conversation where you can ask open-ended questions to the client. After you find out the client is a little more motivated after your discussion, you can draw another line and ask, “How much do you believe in your ability to use a hearing aid?” Again, if they put a low score, you can start discussing why they feel that way. You can take this discussion into a demonstration of a hearing aid; let them manipulate it. The purpose is to start a positive conversation about hearing aids and raise their motivation.
The Box
The box (Figure 2) is just a box with a cross. You can include four things, one in each quadrant. In Figure 2, you see that the quadrants have been labeled Benefits of No Action, Cost of No Action, Potential Cost of Taking Action, and finally, Potential Benefits of Taking Action. It is imperative that the client fill out as much as possible on their own. When they come to a conclusion on their own, it is much better than if you persuade them as to what things are good and what things are bad.
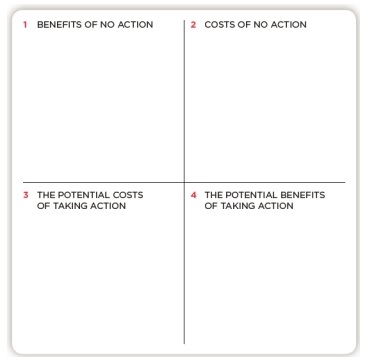
Figure 2. The box motivational tool.
For example, a benefit of no action might be there is not a stigma, because they will not have to wear anything on their ears, pay anything out of pocket, or learn anything new about foreign technology. What are the costs of taking action? The first cost is the physical payment of the hearing aids; that can be a weighty issue for some and should be taken seriously. Another cost could be stigma. They will have to wear it and may not like people seeing it.
What are the potential costs if they do not get a hearing aid? Some costs would be social isolation. They do not get out much and will continue to withdraw because they cannot hear well. People might perceive the client as less attentive because they miss people saying hello.
A third thing that we as audiologists know is auditory deprivation. If someone waits and waits, it will be harder for them to adjust to hearing aids. This is not something they would write down, but you can say that, for some people, it is better to start early.
What are the potential benefits of taking action and getting a hearing aid? They may have a better quality of life, better social quality, or less fatigue after speech communication in noise. When you have listed all this, it is clearer for the client. Are their pros and cons more than just thinking it is too expensive? It will give more variability in the actions you can take.
COSI
Another tool that can be useful in finding out motivation is the Client Oriented Scale of Improvement (COSI). When I use this for discovering motivation to accept amplification, I use the first part where you discover the patient’s specific needs. You have to set up specific situations where the client wants to improve their hearing.
It is not enough to give generalities such as, “to hear better in noise.” Be specific, such as hearing on the phone with a grandchild, or sitting around the dinner table with family. I find that if people with milder hearing loss cannot come up with two or three situations where they want to improve their hearing, they might not experience enough of a problem for hearing aids to be worth the investment.
Communication Management
Whether you find that a person is or is not motivated to get hearing aids, you can counsel about communication strategies. I find this to be almost as important as doing the expectation management. Communication strategies clearly increase hearing aid benefit. Many of us without hearing loss use these communication strategies in our daily lives, and some people with hearing impairment have trained themselves to perform these communication strategies in their daily lives without even knowing it. These are easy and inexpensive ways of improving communication, both with and without hearing aids.
Listening Environment
We can teach our clients what good communication strategies are and what a good listening environment is. If you are hearing impaired, all the reverberations in the room will clearly make the signal poorer for you. If you can choose a room has carpet or wooden walls instead of concrete and not so many windows, it would be of benefit. If you have hearing aids with directionality, the less reverberated signal that enters the hearing aid, the better; then the directionality algorithm can perform better.
Another thing you can teach is about lighting in a room. Always make sure that you can see the face of your communication partner. For example, if the table is in front of a window at a restaurant, as the partner with hearing impairment, you should be the one with your back sitting to the window so you can see the face of your communication partner.
Tell your patients about signal-to-noise ratio. Many people move closer if they cannot hear, but if you are going to a show or presentation and already have a seat purchased in a certain place, it is a bit too late to move closer. If you are aware that more distance means poorer hearing, you may be able to choose seating that will accommodate better hearing.
A good listening environment also means not having excessive noise in the background when you are talking to someone. Why would you have the radio on if you want to have a conversation? If someone is watching the television, go into another room to converse, or turn down the radio or TV. These are beneficial tips for listeners with normal hearing, as well.
Responsibility of the Person with Hearing Loss
What can the listening impaired teach their communicative partners to do? Sometimes a person with hearing impairment does not want to draw attention to their hearing loss, but if they can move past that that because they want to hear what is being said, they can teach their partners to use gestures that will help get their attention before talking. An example would be not talking from the kitchen into the living room. Ask people to talk one at a time. Slow down the communication speed. Speak clearly and naturally. Do not raise your voice; that does not help. Also, be patient. Old habits die hard and relearning a communication style can take time.
The person with the hearing loss should always try and facilitate communication and take ownership of the situation. They should prepare ahead of time if possible. For example, finding out the agenda of a meeting beforehand will help to know a little of what is being talked about. Have good repair strategies of what you can say. Do not be afraid to ask someone for repetition, but be more specific. Instead of just saying, “Huh?” or, “What did you say?” you can say, “Your mother is coming with the train. What time did you say to pick her up?” In this case, the communication partner only has to repeat what the exact time was.
Communication strategies can be used with everyone. If you are fitting a hearing aid to someone, the strategies can be used to improve the benefit of the hearing aid fitting and make the person much happier with the hearing aids.
If someone is being dragged in by their wife or husband to my clinic, after doing all of this motivational communication, I can sense that this person is not ready for hearing aid fitting. In that case, I would still teach them these communication strategies so they can be used until they are ready to do something about their hearing problem. This way, they will think back to the visit at my clinic and realize that I did not try to push hearing aids on them, but that I counseled them on how to improve their communication without getting hearing aids. It is my hope that they will remember that I was knowledgeable professional who treated them with respect, and then will return to my clinic when they are ready.
Mild Hearing Loss Solutions
There are several technology solutions that can be fit for people with mild hearing loss.
Instant-Fit Solutions
Instant-fit solutions can be successfully fitted because the fitting range is perfect. Someone once mentioned to me that instant-fit solutions are like “buying off the rack of clothes.” It fits fine on most people and is appropriate for most occasions, but sometimes it is worth spending more money on a tailored suit. There is nothing wrong with off-the-rack, and they look good in some ears.
There are advantages and disadvantages to instant-fit solutions. They may not be a good fit for everyone. You have to pick the people with the ear that is appropriate for these devices. They may have feedback problems if there is a mild hearing loss that then slopes in the high frequencies and requires a lot of gain.
Custom Hearing Aids
When we have the tailored suit, which are the invisible-in-the-canal (IIC) and the completely-in-the-canal (CIC) custom devices, they can be very appropriate for the mild hearing losses as they are very discrete. The client can also wear glasses, and there is no wind noise. However, there is a risk of occlusion if the impression or hearing aid is not made properly, resulting in a poor fit in the ear canal. Additionally, the insertion and removal has to be trained.
We also have in-the-ear (ITE) devices. They have the same advantages and disadvantages as the smaller ITE devices, however, they are not as discrete in the ear. If you have very small ears, even an in-the-canal (ITC) can look like an ITE, and may not be the most physically appealing device.
Mini BTEs and Open Fittings
Then we have the mini behind-the ear (BTE) and BTEs with open fittings. These would be my go-to device, because they have so many advantages. They look very discrete and fit comfortably on most people. They are also versatile with choices in tube lengths and domes. They are non-occluding and can utilize the ear’s natural hearing since the ear canal is open. They are also transitional. Even if the hearing loss deteriorates over time, you can keep the same device and change the coupling. They have directional capabilities and are compatible with many accessories. With thin tubes and pliable domes, they are good for even narrow ear canals.
One disadvantage could be that the microphones are positioned behind the ears, which may cause a delayed signal or echo in the ear, although many manufacturers have accounted for this in the signal processing. Also, if you have ears that lie very close to the head, you could encounter problems with patients who wear glasses. Insertion and removal might need to be trained, but a first-time user with any device would also need some training.
RITE
Much like the open BTEs and mini BTEs, there are receiver-in-the-ear (RITE) devices. They have all the same advantages as the open fitting, but they can be slightly smaller, as the receiver has been moved into the ear canal instead of sitting in the device on the back of the ear. They are a little more prone to repairs because the receiver sits in the ear canal and can be affected by wax and moisture. Also, for the very narrow ear canals, you may not be able to fit all manufacturers’ receivers. Additionally, I have encountered a few people in my clinic who have good hearing in the low frequencies and they could hear the receiver noise. I had to fit them with a thin tube instead. Finally, a RITE costs more than a thin-tube device.
Standard BTE
What do you think about a standard BTE? As a first choice, I would not choose a custom earmold for mild hearing losses because there is a high risk of occlusion. The size of the device can also be a hindrance for those concerned with cosmetics. I would start with a RITE; if there was a need to close the ear canal, I would try a RITE with a power dome or a custom mold. If you have people with skin allergies, you may have to do a custom earmold. I have seen gold-plated and even titanium earmolds as hypoallergenic options.
What is the Best Way?
Programming
Many manufacturers offer a proprietary first-time fitting rationale that provides less initial gain, which can be helpful as long as you remember at the next visit to turn up the gain to match targets. Some people with mild hearing losses do not need that much gain to satisfy their hearing needs. I would start with a first-time-use fitting, and then increase the gain no later than two or three weeks later. That would be a good way to ease them into the gain that they need.
Feedback management
For open fittings, you will need to turn on the feedback management system, but make sure that manufacturer’s system does not turn down gain in any situation where the hearing aid would whistle. This group does require that much gain anyway, and there is no reason to turn it down. If they put their phone up to their ear and the system turns the gain down, they might as well not have the hearing aid on.
Directionality
Directionality to improve the signal-to-noise ratio is recommended. In most current hearing aids, you can use an automatic switching program that would go into directionality when needed rather than having multiple manual programs.
Noise Reduction
Noise reduction does not improve the signal-to-noise ratio, but it is a comfort feature. That is important for this group, as we want them to accept the hearing aids. We do not want them to feel that it is noisy.
Counseling
There are many different ways of counseling new users with mild hearing losses on how much they need to wear the hearing aids and in what situations they should be worn. As a matter of observation, audiologists say vastly different things from one clinic to the next. Normally, I encourage them to wear the hearing aids as much as possible in order to make the transition faster. I have also had success with people only using the hearing aids in the situations where they need them.
Asymmetric Hearing Loss
I wanted to mention asymmetric hearing loss. We have students doing a case study in-house with people with severe hearing loss on one side and mild hearing loss on the other side. Their findings showed a slight tendency to prefer the open fitting on the ear with the mild hearing loss and a closed fitting on the ear with severe hearing loss. A few people preferred closed fitting on both ears, and that came as a surprise to us.
It really is up to the individual. If you have the time and opportunity, you should try both and have the person tell you what they like the most. There was also a preference for the fitting that gave the best speech-in-noise score as the preferred fitting.
Wireless Accessories
Do the people with mild hearing losses need wireless accessories? A TV will turn up in a linear manner, and a TV streamer will turn up according to the hearing loss. I would not fit a person with a mild hearing loss with a TV Streamer at the initial visit. If they came back and complained that they still had problems hearing the TV with the hearing aids, I would offer it to them. However, the TV Streamer may be like using a sledgehammer to crack a nut.
An external microphone, on the other hand, tackles the background noise that many hearing aid users experience with the hearing aid, as it picks up the signal at the speaker’s mouth and sends it wirelessly to the hearing aids. We did a study to see that, over increasing distance, the directionality program in the hearing aids will create a worse signal-to-noise ratio score. However, when you clip an external microphone on the talker, the signal stays strong, even as you move further away. Just as with the TV streamer, I would not dispense an external microphone to a person with a mild hearing loss until they complained about background noise with hearing aids.
Not being able to use the phone impacts quality of life (Dalton, Cruickshanks, Klein, Klein, Wiley, & Nondahl, 2003). Many people report that if they cannot use their hearing aids on the phone, they probably will not use them at all (Kochkin, 2000).
When speech is transmitted to both ears instead of one, there is a significant benefit. This can be done through a phone clip that is coupled to the hearing aids and the phone. It will stream the signal from the phone to the phone clip and then from the phone clip to both ears. You can also have the phone signal streamed directly from an iPhone up to the hearing aids without an intermediate streamer. You can have all the video chatting, music, movies, audiobooks, navigation, and anything else from the phone streamed bilaterally up to the hearing aids.
Anyone who struggles with hearing over the phone would benefit from a streamer or made-for-iPhone device. Ultimately, I would start with hearing aids only and fit accessories based on what they come back and report to you.
Common Fitting Errors
Not Offering a Trial
One common error is when we think a hearing loss is so mild that the client would not get any benefit from amplification. If a patient is motivated, why not try out hearing aids? Here in Denmark, we get free hearing aids. Sometimes the audiologists that would decide who can get free hearing aids or not would say a hearing loss was so mild that the person would not benefit from amplification. That is such as shame because if the person is motivated, he may get benefit in some situations that are important to him had he tried amplification.
Amplify Everyone
Another error is thinking that any degree of hearing loss, even the mildest of hearing losses, requires amplification in any situation. Here, we can turn it around and say that if the person is not motivated, there is a small chance of success with hearing aids. There is a risk that if you push hearing aids and the client does not get the benefit that you promised, they would never come back to you.
Directional Benefit for Open Fittings
Another fitting error is assuming there is no directional benefit for open fittings. Some factors that influence directionality are the location of the sound source, location of background noise in the room, spacing between the two microphones on the hearing aid, and how well the microphones in the hearing instruments are matched. We also know that low-frequency sounds are more omnidirectional, and high-frequency sounds are more directional. Low-frequency sounds will not reach the mildly impaired hearing aid user using open fits, but the higher frequency sounds would.
When the source of interest is in front and the competing noise is in the back with low reverberation, the mildly hearing impaired person could benefit from directional microphones, even in an open fitting. There is no reason not to put it on; just remember to adjust your expectation management when you have an open fitting.
Fitting Configuration
Another error is not telling the fitting software which fitting configuration you are using. Some manufacturers compensate the acoustic fitting based on what instrument, tubing and/or earmold you use. The vent size, or openness of the ear canal, has a direct effect on directionality. Dillon (2012) showed that an occluded fitting has a relatively flat response with no more than 5 dB vent attenuation, while a fitting with a tube with no earmold (open canal) can affect the low frequencies by 25 to 30 dB and even the mid to high frequencies by 10 dB. Make sure you tell the software the physical characteristics of the hearing aid and venting.
In-Situ Testing with Modifications
Another error is not performing recalibrations when you change tubing, hooks, or domes. For instance, if you have a tulip dome and you do your calibration (real-ear measurement), the fitting software will show a graph of how high you can turn up the gain without being at risk for feedback. If the person then says they feel occluded, you can try an open dome, but you have to check the in-situ fit again.
Figure 3 shows the difference between a hearing aid with an open dome and a hearing aid with a tulip dome. You can see there is much less stable gain for the tulip dome. However, if you do not do the recalibrations, you will not know this. The feedback manager will act differently than you think, and you might end up not understanding why the patient has feedback problems.
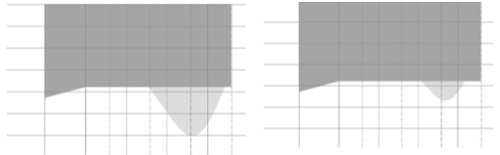
Figure 3. Differences in stable gain between an open air dome (left) and a tulip dome (right).
Follow Up
The last error is thinking that fitting a hearing aid is the complete solution and your job is done once the fitting is complete. This is not true. It is important to counsel, educate on communication strategies, and do expectation management.
Conclusion
Thank you for your attention today. My hope is that these strategies and tips will help you to feel more confident when fitting patients with mild hearing losses.
Questions and Answers
Do you recommend open molds for mild hearing loss the majority of the time?
Yes, I do. I fit with open domes initially, especially if it is a first-time user. If there is a need for a more closed fitting, I would gradually change from an open dome to a tulip dome to even a custom mold if the patient required it. Little by little allows them to adjust.
References
Clark, J. G. (1981). Uses and abuses of hearing loss classification. Asha, 23, 493-500.
Cox, R. M., & Alexander, G. C (1995). The abbreviated profile of hearing aid benefit. Ear and Hearing, 16(2), 176-186.
Dalton, D.S., Cruickshanks, K. J., Klein, B. E., Klein, R., Wiley, T. L., & Nondahl, D. M. (2003). The impact of hearing loss on quality of life in older adults. Gerontologist, 43(5), 661-668.
Dillon, H. (2012). Hearing aids, second edition. New York, NY: Thieme.
Dillon, H., Cameron, S., Ching, T., Glyde, H., Keidser, G., Hartley, D., & Mejia, J. (2010, August). Mild hearing loss is serious business. Presentation at the International Hearing Aid Research Conference, Lake Tahoe, NV.
Hougaard, S., & Ruf, S. (2011). EuroTrak I: A consumer survey about hearing aids in Germany, France and the UK. Hearing Review, 18(2), 12-28.
Kochkin, S. (2009). MarkeTrak VIII: 25-year trends in the hearing health market. The Hearing Review, 16(1), 12, 14, 16, 18-20, 22-24, 26, 28, 30-31.
Kochkin, S. (2000). MarkeTrak V: “Why my hearing aids are in the drawer”: The consumer's perspective. The Hearing Journal, 53(2), 34-41.
Mecklenburger, J. & Joergensen, S. (2009). Presentation at the American Academy of Audiology Conference, Dallas, TX.
World Health Organization. (2012). WHO global estimates on prevalence of hearing loss. Retrieved from https://www.who.int/pbd/deafness/WHO_GE_HL.pdf
Cite this Content as:
Moeller, K.N. (2015, January). The mild misnomer: diverse needs for mild hearing impairment. AudiologyOnline, Article 13180. Retrieved from https://www.audiologyonline.com.

