
Editor's note: This course is an edited transcript of a live webinar. Download supplemental course materials.
Learning Objectives
Anne Mette Jeppesen: Welcome to this presentation called “Empower Patients to take Action on their Hearing.” This is a presentation about the Ida Motivation tools.
The objectives for this course are that learners will be able to explain how to empower patients to express their needs and concerns in a structured dialogue, explain how to uncover patient’s internal motivation for taking action and address ambivalence, and explain how to use three Ida Motivation tools in their own practice.
In hearing care, when we try to encourage more people to seek help for their hearing, we often use external motivators like discounts or celebrity endorsement, but it turns out that the most powerful source for change and fuel for sustained change is internal motivation. With this presentation, I will try to help you understand how patient readiness effects decision making in the consultation and how patient uncertainty or ambivalence should be seen as an essential part of the change process that the patients go through. I will introduce you to the Ida Motivation tools: the lines, the circle, and the box, which are three tools that support the decision making process in the clinic.
Ida Institute
The Ida Institute is an independent, non-profit organization that was established in 2007. It is funded by the Oticon Foundation, and it is a global organization with about 7,000 members. All of the Ida tools and resources that we have freely distributed, including what I will talk about today, are publically available at our website (idainstitute.com). Since 2014, the Ida Institute has had a strategic partnership with William Demant.
The mission for the Ida Institute is to foster a better understanding of the human dynamics associated with hearing loss. The reason why we have this mission is that, despite the fact that technology has improved a great deal the last 10 years, and the fact that there is a growing number of people with hearing loss, we do not see a greater uptake of hearing aids or services to help overcome the negative consequences of having a hearing loss. Because of that, we believe that we need to place more focus on the human dynamics of hearing loss if we wish to enable more people to seek help and act on recommendations.
The way we work at the Ida Institute is through collaboration. You could say that collaboration is at the heart of all our initiatives. We collaborate with our global community to understand the challenges within the field of audiology. We explore solutions together with our community and then we create tools, methods, and processes that are needed within the field of audiology. We try to meet the unmet needs in audiology by creating tools for audiologists by audiologists.
Ethnographic Videos
One of the tools we use to understand needs within audiology are ethnographic videos. These videos depict real-life situations at the clinic and in the homes of persons with hearing loss. They provide a unique insight into audiological practice and the challenges hearing impaired individuals face in their daily lives. Further, they give hearing care professionals a chance to reflect on situations that happen and exist in the real world. In the films, you see audiologists reflect on their experiences, and you also see patients reflect on their hearing loss in a way that is often uncommon during a typical consultation. The films offer a valuable outside peek into the patients’ and the communication partners’ perspective on having a hearing loss.
It is important to know that when we watch these videos it is not our intention to be critical towards the audiologists, patients or families. It is to help hearing care professionals reflect on clinical practice and help them think about how they can become more patient-centered.
I would like to show you one of these ethnographic videos. This one has been reenacted verbatim by actors to protect the privacy of the participants. The tenor of the encounter is preserved in the reenactment in order to reflect the real-life situation as closely as possible. When we watch this video, I would like you to pay attention to what happens during the clinical encounter between the audiologist and the patient and think about what dilemmas are facing both the client and the audiologist.
When I watch this video, I notice how the audiologist and the patient seem to speak to different languages. The audiologist speaks a lot about audiograms, pure tones, frequencies, and hearing aids at the end, which we did not see here. The patient speaks about how she cannot hear her husband, how he is deteriorating, and how she cannot hear her grandchildren or her neighbor. Then she talks about her sister’s experience. The patient speaks a lot about those things that matter to her, but it is like the audiologist does not really hear her. She does not address the patient’s ambivalence and does not seem to understand the patient’s concerns.
If we look at the dilemmas the audiologist is facing, it seems as if she has her own program that she wants to carry through. She seems to be under pressure to finish the appointment within the given time, and then she really wants to demonstrate that hearing aids will do the job and solve the patient’s issues.
If we then look at the dilemmas facing the patient, her husband has Parkinson’s disease and he speaks very quietly, which she cannot hear. She struggles to hear her grandchildren and the neighbor on the phone. She is concerned about the cost of the hearing aid. Even though she says she would wear a pin saying Hard of Hearing, later on she mentions that the audiologist does not have a hearing aid that matched the color of her hair. She is a bit concerned that people will be able to see the hearing aids if she wears them.
When I look at this encounter, there is a mismatch between the two and how they communicate with each other. It seems as if the audiologist does not listen to the patient to find out what her needs are. When looking at this clinical encounter, I think that most of us can recognize situations like these. What could we do to change the way we interact with our patients and become more patient-centered? Can we do something to listen to the patient’s needs and address their concerns and their ambivalence?
Motivational Engagement
Motivational engagement is a person-centered approach. It is a means to identify where the patient is in their journey. It can help us build a dialogue and reach core issues in limited time. It lets the patient do the talking so that we can uncover their internal motivation. As audiologists, we have a tendency to think that patients need the same information that we do, and if they have come to see us, they must be ready to carry out our recommendations. If we provide clear and detailed information about the patient’s hearing loss and options for treatment, we often believe that patients can act more easily. However, we have to realize that when we ask patients to follow our recommendations, whether it is wearing a hearing aid or asking them to change their behavior, we are expecting them to change their daily habits.
Changing habits is hard. We know this from other areas like losing weight or getting adequate exercise, and within the medical field, taking vital medication or controlling sugar intake is difficult. If we look at audiology, that is the same thing. We know that it is difficult for people to use their hearing devices, and it is also difficult to adopt effective communication strategies. Even though people know what is best for them, it is not automatically followed by doing.
As professionals, we often try to persuade the patients to change their habits. We do that by giving information and making recommendations. However, information and recommendations rarely work well. Patients fail to follow the recommended practice, and they may even drop out of treatment, and that leaves us, as professionals, feeling frustrated or dissatisfied. Instead of persuading the patient, it is so much better to let the patient convince themselves of the need to change. It is more effective, and we know it has a longer lasting impact. It also utilizes professional expertise and time more effectively.
How do we do this? Motivational interviewing is a protocol that can be used to increase patient adherence to audiologist recommendations. It is a patient-centered counseling approach that can help us better understand our patient’s perspective. Within this approach, the patient does most of the talking, and the interaction between the clinician and the patient is thought of as a meeting between experts. The practitioner is the expert on the disease, and the patient is the expert on their life and how they are affected.
Within motivational interviewing, lack of motivation on a patient’s behalf is seen as a state that is open to change. Motivation is not an all-or-nothing thing. It is something that we can help them change. The way motivational interviewing facilitates this change is by helping the patients explore and resolve their ambivalence about the behavior change.
From this perspective, the clinician and the client both play a very central role. The patient’s task is to articulate and resolve his or her own ambivalence with guidance from the practitioner. The practitioner’s task is to expect and recognize ambivalence and then to be directive in helping the patient examine and resolve this ambivalence.
What does it mean to be directive? It means that we need to address the ambivalence in a structured way, and we can do that by using tools to help guide the patient in understanding their own ambivalence.
Changing Habits
Changing habits is fundamental in audiology. Whenever we recommend something, we ask our patients to change their habits. When people change habits, they follow a very well-recognized pattern. We have some simple tools that can support this change process. The first of these tools is the Circle (Figure 1), which is based on the Stages of Change Model developed by Prochaska and DiClemente (1983).
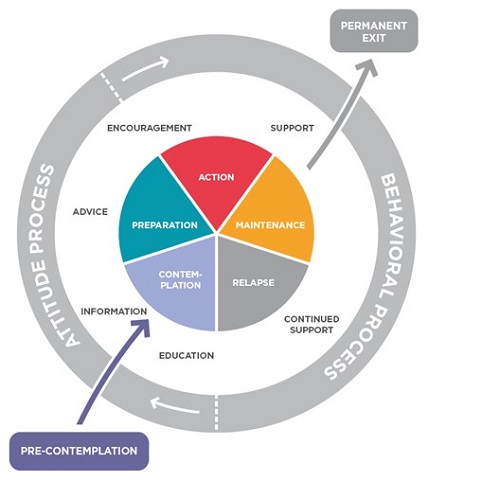
Figure 1. The Circle.
The Circle can be seen as an intervention guide. It is a tool that the clinician uses to identify the client’s readiness to change and to help the clinician decide how to support the patient. The circle looks at personal change as a process. First, a person needs to change their attitude and then they move on to changing their behavior. That is shown in the gray circle.
Within these two processes, there are seven different stages a patient undergoes when changing behavior. They start out in pre-contemplation, then they move to contemplation, preparation, action, and to maintenance. From maintenance, they either go to permanent exit or to relapse. Depending on what stage the patient is in, you should tailor the information you provide to the patient’s needs.
There are different ways to respond to the patient, and those can be seen in the white circle (Figure 1). Again, the circle is meant to be a clinician intervention guide, and it can help the clinician find out at what stage of change their patient is in and how to help the patient. Let’s go through the stages in more detail.
Pre-Contemplation
The first phase is what we call pre-contemplation. A patient at this stage does not realize or believe that he or she needs to change. This is a person who was brought in by a spouse or a child. A patient in this phase considers comments and information on their hearing loss as irrelevant or misplaced or interfering. A patient at this stage would typically make excuses for their own behavior. They are quite surprised when they are presented with others’ perceptions of the problems. The best thing for the professional to do in this phase is to listen to the patient and then only provide clear, short, and exact information. We do not want to give them a lot of information or advice at this stage. They are not ready for those explanations.
Contemplation
The next phase is contemplation. At this stage, the patient feels comfortable with his or her present habits, but they have also started to be a little bit afraid of the consequences of continuing with the present habits. A patient in this stage will typically resist the idea of changing habits, but they also want to change. You see a lot of ambivalence at this stage. The best way the professional can support the patient is to listen to the patient, start to explore his/her experiences with hearing and communication, and maybe give some brief advice regarding possible options for improving hearing and communication. Then you would support and acknowledge the patient’s increasing awareness of the ambivalence.
Preparation
The next stage they move into is preparation. As the patient moves into this phase, they will continue to express ambivalence, but they will have reached a tipping point and decide to act on the hearing loss. However, they are not sure how to proceed. The patient will seek information to back their decision and will look for backing from the audiologist and also from others to find out if they should go in this direction. The patient starts to show motivation at this point and seems to be ready to take some sort of action on their hearing loss.
At this stage, the role of the audiologist changes a bit. It is still helpful for the audiologist to support and listen to the patient, and then to support the patient in planning the use of new strategies. At this stage, we can also start to give the patient some advice and ideas about what it takes to improve communication with others. However, it is still important not to present the one and only solution, because they may not be ready for this. If we do that, we might force them in the wrong direction. A good thing to do is to focus on the benefits of better hearing and use that to encourage the patient to move on further in this direction.
Action Phase
A patient in the action phase is now moving forward. The patient is happy and proud of doing this. He/she talks about the change and looks for acknowledgment and appreciation. Very often, he/she feels that it is not as difficult as they expected. Once they reach this step, they seem to feel a lot of success. At the same time, they are often a bit worried about giving up the change and relapsing. With a patient at this stage, the professional should listen to the patient and focus on the personal benefits of improved hearing and communication, and then again encourage and support the patient in what they are doing.
Maintenance
The patient has now become a hearing aid user and/or is using effective communication strategies. The patient is still ambivalent, however. He is pleased to have taken the step to become a hearing aid user, but he also finds it hard to accept the implications of the hearing loss. Often, he will see the hearing aids as a necessary evil. He feels sad from time to time and forgets why he wanted to change behavior. At this stage, the patient either feels successful with using the hearing aids and communication strategies, or they could feel that they want to give up. If they feel successful, it will lead to permanent exit. Feeling despair will lead to relapse.
Relapse
If the patient gives up, he goes in the relapse phase. Here, the patient will feel like a failure. At the same time, he might relax and enjoy the freedom of old familiar habits. Very often, the patient will be angry and annoyed at himself, and feel that he is being of weak character. When a patient is in this stage, they might be motivated for new attempts regarding changing habits again. Even though they have ended in relapse, it is not that they have not moved anywhere. If they are motivated to go for another attempt, they do not necessarily have to start all over. They might be able to jump right into the action phase and then move on from there.
When a patient is in a this phase, the professional should try to focus on the advantages of better hearing and communication, and then focus on the manageable steps that enabled the patient to previously implement new strategies. Even though the patient did fail, we try to look at the successes that they had.
We want the professional to put focus on positive experiences, even if they were only for a short duration. They should try to make the patient agree on a new habituation scheme. Again, we support as much as possible and we listen.
Permanent Exit
If, on the other hand, the patient feels successful in the maintenance phase, he or she will move into the permanent exit phase. A patient at this phase feels safe and comfortable with the new behavior and has fully integrated the new habits into his or her lifestyle. At this stage, the professional will provide the possibility to return for support. Hopefully the patient will be successful and independent while enjoying the hearing aids.
The circle can help you identify where your patient is in relation to the changing process. It can help you know in which ways you can support the patient through this changing process.
Identifying Stages
How do we identify the stage the patient is in? A very simple way of doing this is to ask the patient to identify which of the five statements listed below applies to them:
- I am not ready for hearing aids at this time. (Pre-contemplation)
- I have been thinking that I might need hearing aids. (Contemplation)
- I have started to seek information about hearing aids. (Preparation)
- I am ready to get hearing aids if recommended. (Action)
- I am comfortable with the idea of wearing hearing aids. (Maintenance)
This is a very easy way to find out where you patient is in the circle. Then use the circle to guide you on how to best support the patient.
If we think back to the patient that we saw in the video and how she would have replied to the questions above, my guess is that she would have probably answered that she thinks she may need hearing aids and she has been seeking out information on hearing aids. She is quite ready to learn more about it when she enters the clinic. From the audiologist’s perspective, if she had had this information, that would have made it easier for her to help the patient go through the stages of change. If we look at the video and we think about the patient to begin with and then we think about her at the end of the video, it seems that the audiologist was not able to bring her in the right direction through the stages of changes, but one might argue that the patient actually went backwards. At the end, if she was asked, she probably would have replied that she was not ready for hearing aids at this time.
The Lines
The next tool I will share that also supports the change process is the Lines (Figure 2). The Lines provides a structured way to guide dialogue with the patient. They are designed to help assess the patient’s perception of how important it is to improve their hearing and how strongly they believe in their own ability to make the required changes, such as beginning to wear hearing aids or change their communication habits. As such, the Lines present a quick way to get to the core of the patient’s motivation and concerns, and then help make efficient use of the clinic time.
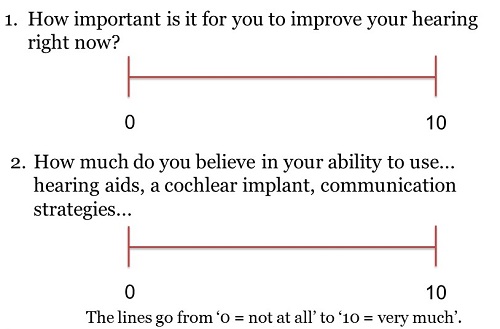
Figure 2. The Lines.
These simple visual analog scales range from 0 to 10, where 0 means Not at All and 10 means Very Much So. The first line asks the question, “How important is it for you to improve your hearing right now?” The second asks, “How much do you believe in your ability to use hearing aids, cochlear implants, etc.?” Ask the patient to put a mark on each line to describe their current standpoint in relation to the two questions asked. This is a simple and useful way to create a shared understanding of the importance to change the habits and the confidence or self-efficacy of the patient. It also gives the patient time and space to reflect on their issues, which might be the first time they have ever done so. The Lines are most useful for patients who are in contemplation or preparation. However, they can be used throughout the fitting process to track the patient’s changing views and also to monitor progress.
When you ask the patients to put their marks on the Lines, ensure that you give the pen to the patient and have them do it without input from family members that may be there. Once the patient has put their marks on the lines, you can begin to explore why he or she placed their marks the way they did.
For example, if they scored themselves low, you can ask why they did not score themselves higher or vice versa. By articulating their reasons to you, the patient is required again to think about their motivation for improving their hearing and also their belief in their own ability to do so. This is an important step in the decision making process. People are more likely to be convinced by listening to their own arguments than those presented by others. By giving them these Lines and starting to explore why they put the mark where they did, we give the patients a chance to express themselves and bring forth their own arguments for creating the change.
We do not stop there. Instead, we dig deeper by asking what it would take for the patient to increase their score from A to B. We ask the patients to reflect on their own situation and how they think about making the change.
When you do this, you may find that they have some concerns that prevent them from moving forward that they would not have mentioned had they not been prompted to do so. I am guessing that the patient in the video would have scored somewhere between 8 and 10 when asked how important it is for her to improve her hearing right now. She was quite motivated to improve her hearing when she entered the clinic. On line 2, I suspect that she would have placed the mark a little lower, somewhere between 4 and 6, primarily because of her experience with her sister. If the audiologist had seen this picture, it could have helped her dig deeper into the patient’s ambivalence and also address the issues the patient experienced.
The Box
The last of the three motivation tools is called the Box (Figure 3). This tool is for patients who rank their motivation for change low on the Line, and are in the pre-contemplation or contemplation stages in the Circle. The Box is a strong visual tool that can help patients organize the pros and cons of taking action versus not taking action on their hearing loss. As we have seen, the ambivalence many patients feel towards making the required changes is a very normal part of their decision-making process. The goal of the Box is to help guide patients through consideration of the cost and benefit trade-off between getting hearing aids and not getting hearing aids.
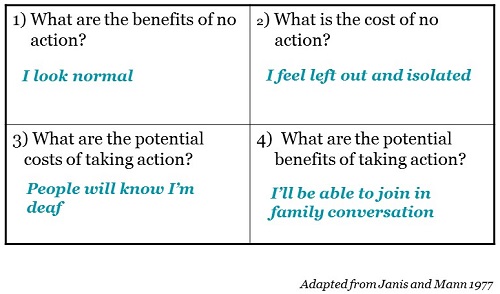
Figure 3. The Box.
It contains four simple questions to help us see issues that are deemed negative and positive for the patient. It starts as a structured way to think about pros and cons. The first questions is, “What are the benefits of no action?” Then you ask, “What is the cost of no action?” The next question is, “What are the potential costs of taking action?” Finally, “What are the potential benefits of taking action?” As much as possible, you should have the patient fill in their answers themselves, and make sure to leave sufficient time for them to think about their answers. Most often you will find that seeing the pros and cons in such a structured way will help the patient in their decision making process and they will more often than not begin to see the benefits of taking action on their hearing problem.
Let’s look at some possible answers on the four questions. One benefit of no action could be, “I look normal.” One answer to “What is the cost of no action?” could be, “I feel left out and isolated.” The answer to “What are the potential costs of taking action?” could be, “People will know I am deaf or hard of hearing”, and the answer to “What are the potential benefits of taking action?” is, “I will be able to join in family conversations.”
If we think about our patient in the video, she would have probably said that the benefits of no action are that no one can see she has a hearing loss, she will not need to spend money on hearing aids, and she will have no trouble handling technical problems as her sister experienced. The costs of no action for her would be that she cannot hear her husband, grandchildren or neighbor on the phone. The potential costs of taking action could be technical trouble with the hearing aids and people will see that she has a hearing loss. The potential benefits for her in taking action could be hearing the important people in her life and help her husband better.
I would like to show you a video of a clinician trying out the Lines tool in the clinic. Then we will hear her reflections on how she felt and what it was like using this tool.
In this video, Naomi saw quite a few benefits of using the tool to structure the dialogue, and that it gave her a chance to understand the patient’s needs and concerns, instead of going with her preconceived ideas about the patient. Besides these comments, which are typical from audiologists that have used the tools in the clinic, they also often report that listening more to the patient allows them to provide better solutions. They have reported they have felt time savings by getting to the heart of the issue upfront and more meaningful interactions with clients. They also report improved job satisfaction because many of them feel they are better able to help the clients with their needs and concerns.
Summary
In summary, taking action on hearing equates to changing habits. Internal motivation is the most powerful source for changing these habits and for behavior change in general. Motivational interviewing facilitates behavior change, and the three Ida Motivational tools can be used to empower patients to take action on their hearing and make appropriate behavioral changes. The Ida Motivational tools consist of the Circle, the Lines, and the Box.
Reference
Prochaska, J., & DiClemente, C. (1983). Stages and processes of self-change in smoking: toward an integrative model of change. Journal of Consulting and Clinical Psychology,5, 390–395.
Cite this Content as:
Jeppesen, A.M. (2015, May). Empower patients to take action on their hearing, presented in partnership with the Ida Institute. AudiologyOnline, Article 14031. Retrieved from https://www.audiologyonline.com.

