Learning Objectives
After this course, readers will be able to:
- Explain the importance of a comprehensive management program for tinnitus.
- Identify outcome measures used for assessing the effectiveness of tinnitus management programs.
- Describe the contribution of various components of a tinnitus management protocol used to reduce tinnitus distress.
Background
Tinnitus is a perception of sound in the ears or head in the absence of an actual physical sound. Tinnitus represents one of the most common and distressing otologic problems, and it can cause various somatic and psychological disorders that interfere with the quality of life (Yetiser et al., 2002). Approximately 12 million individuals in the United States have been diagnosed with tinnitus, of which ~1 million have severe tinnitus interfering with their daily activities (Meikle, 1997; Tyler & Baker, 1983). Various treatment methods from medications to electrical stimulation to alternative medicine have been investigated, but all have limited efficacy at present. These treatments are generally aimed at reducing or eliminating the tinnitus perception, and have been largely unsuccessful in that goal.
Sound therapy is a widely used and accepted method of managing bothersome tinnitus. The goal of sound therapy, along with counseling, is to reduce the distress associated with tinnitus and to encourage the process of habituation, rather than attempting to eliminate the perception. The efficacy of sound therapy has been documented in numerous studies, but remains unclear due to numerous variations in types of sound therapies and lack of controlled studies (Hobson, Chisholm, & El Refaie, 2012; Hoare, Searchfield, El Refaie, & Henry, 2014). The proposed underlying mechanisms for this effectiveness include the reduction of the perception of the tinnitus through masking or partial masking (Henry et al., 2006), the lowering of the gain of the auditory system by adding supplementary auditory stimulation (Formby, Sherlock, Gold, & Hawley, 2007), and decreasing emotional reaction through counseling (Jastreboff & Hazell, 1998). At least one sound therapy program with documented efficacy uses music along with broadband noise as its stimulus (Hanley and Davis, 2008). The addition of music is thought to enhance the effects of sound therapy by working with the limbic system to induce relaxation.
The stimulus for sound therapy is typically delivered through wearable devices for ease of use and mobility. In order to achieve results, the patients must use the sound therapy on a consistent basis, varying between two and eight hours a day depending on the particular program. We now have a number of hearing aid/sound therapy combination devices available on the market to address both hearing loss and tinnitus. Amplification alone has been shown to be quite effective in reducing tinnitus perception in those with hearing loss. (Kochkin & Tyler, 2008) Most of these sound therapy approaches also include a counseling component in the form of informational and sometimes directive counseling or cognitive behavioral intervention. In fact, cognitive behavioral therapy (CBT) alone has been shown to be effective in alleviating tinnitus related distress (Martinez-Devesa, Perera, Theodoulou, & Waddell, 2010). This is understandable as it is well-accepted that tinnitus distress is highly correlated to negative thoughts, fear, and stress, which can be somewhat relieved through CBT.
The importance of addressing the emotional component associated with tinnitus cannot be overstated. There is strong objective evidence that supports the involvement of the limbic system in the overall tinnitus problem (Lockwood, Salvi, & Burkard, 2002). A recent single case study, in which circumstances allowed direct measurement of brain activity in a tinnitus patient, showed involvement of almost all of the auditory cortex, plus large parts of the temporal, parietal, sensorimotor, and limbic cortex (Sedley et al., 2015). This study is further evidence that thoughts, emotions and memory play a part in the tinnitus problem. The emotional component is what differentiates a “person with tinnitus” from a “tinnitus patient”.
Widex introduced a fractal-based musical chime as a sound therapy tool in 2008 (Kuk & Peeters, 2008) This music chime is an alternative to broad band noise that incorporates the benefits of music but avoids its potential limitations by using fractal tones. Auditory fractal tones utilize harmonic, but not predictable, tonal relationships to create a pleasant musical stimulus intended to be relaxing but not repetitive. The Widex hearing aid has the option to include amplification alone, fractal tones, white noise, and narrow band noises of adjustable bandwidths. Each of these options can be used independently or in combination with the microphone amplification turned on or off. Previous studies with fractal tones (Sweetow & Sabes, 2010; Herzfeld, Ciurlia-Guy, & Sweetow, 2014; Johansen, Skellgaard, & Caporali, 2014; Sweetow, Kuk, & Caporali, 2015) reported favorable results reducing the tinnitus annoyance or tinnitus severity in subjects with significant tinnitus.
Later, Widex recognized the need for a complete tinnitus therapy program to address not only the tinnitus perception but also the emotional reaction to tinnitus. Based on the success of the Zen tones, they developed a Widex Zen Therapy (WZT) protocol comprised of four main components:
- Counseling. Both instructional and adjustment-based counseling, with the goals of educating the patient and modifying the negative thoughts and feelings about the tinnitus via cognitive and behavioral intervention.
- Amplification. To provide additional input to the auditory system in order to minimize increases in central activity (overcompensation) and maladaptive cortical reorganization.
- Zen sound therapy options. These options include fractal tones as described above, along with broadband noise, and/or filtered broadband noise.
- Relaxation strategy program. Relaxation exercises with demonstration exercises and a take home CD, along with sleep management strategies.
The studies cited earlier in this paper examined the usefulness of the Zen tones, or the overall effect of the WZT program as a whole. The aim of this study was to evaluate the relative contribution of each component of WZT in reducing tinnitus distress. Such information may be helpful to practitioners seeking the most effective and efficient methods to alleviate tinnitus distress in their patients.
Methodology
Twenty adult subjects were enrolled in this study. All had significant tinnitus disturbance defined by a Tinnitus Functional Index (TFI) (Meikle et al., 2012) score of >38, with a tinnitus onset >6 months prior to enrollment. Using the TFI guidelines for evaluating tinnitus impact at intake, (Henry et al., 2014), we separated the subjects into 3 groups according to severity: five subjects had a “moderate problem” (TFI 32-53), eight subjects had a “big problem” (TFI 54-72), and four subjects had a “very big problem” (TFI 73-100). One subject had normal hearing, four subjects had minimal hearing loss (normal through 2 kHz) and, 15 had hearing loss less than 70 dBHL at any one frequency. Only one subject had previous hearing aid experience. Significant anxiety or depression was an exclusion criterion.
Subjects were seen for eight visits over a 12-month period. The Widex Zen Therapy protocol was followed. Devices used were the Widex Clear 440 Fusion, a premium, digital, receiver-in-the-ear style hearing aid with the ability to provide customized Zen tones and/or broadband noise as sound therapy. For patients with normal hearing or minimal hearing loss, the device was programmed with minimal or no amplification. The four components of WZT - instructional counseling, amplification (for those with hearing loss), Zen tones, and adjustment-based counseling (including cognitive behavioral intervention or CBI, relaxation exercises and sleep hygiene as needed) - were provided to all subjects sequentially at two-week intervals. The adjustment-based counseling component was provided at one or more appointments, as determined by patient needs.
Outcome measures at each two-week interval included the TFI and several visual analog scales (VAS). The Tinnitus Functional Index is a 25-item self-assessment questionnaire specifically designed for responsiveness to treatment. It has eight subscales to measure various dimensions of the tinnitus problem: Intrusive, Sense of Control, Cognitive, Sleep, Auditory, Relaxation, Quality of Life, and Emotional. The score is expressed as a percentage with 100% being the most severe.
The visual analog scales (VAS) used a 0 to 10 scale with 10 being the most severe rating. Five VAS scales were used. Subjects were asked to rate their tinnitus severity, awareness, annoyance, as well as their general level of relaxation and sensitivity to loud sounds.
Data logging was used to measure usage of amplification and Zen tones. Additional outcome measures were completed only at the pre- and post-study sessions; these included minimal masking levels (MML) and loudness discomfort levels (LDL). At the end of the study, subjects were given a questionnaire to rate their perceived overall benefit of participation in the study and the benefit of each WZT component (Appendix A).
Results
Change in Overall TFI Scores Over Time
Although all 20 subjects completed the study, three were eliminated from the data analysis due to non-compliance (did not use the devices, missed numerous appointments). The mean TFI scores after each WZT component over time is reported in Figure 1. For example, “HA use” reflected the TFI scores after hearing aids were used for two weeks. Overall, the mean TFI score improved 28 points from 62 points at baseline to 34 points at the 6 month visit. A change of 13 points or greater on the TFI is considered significant (Henry et al., 2014).
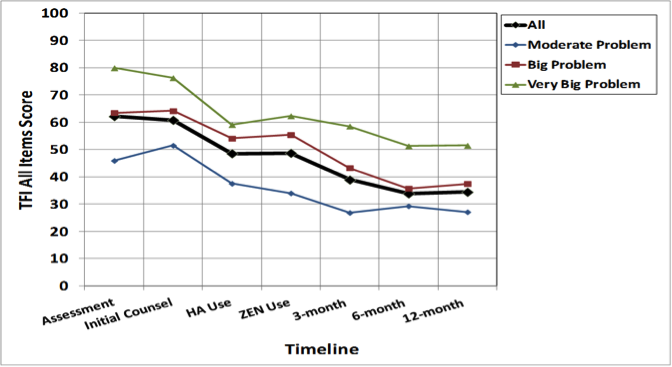
Figure 1. Changes in absolute TFI scores following each individual WZT component.
Initial instructional counseling. This counseling provided general information about hearing, hearing loss, tinnitus and benefits of sound therapy. There was no significant change in the mean TFI scores when administered 2 weeks later (62 points to 60 points).
Amplification or HA use. Clear 440 Fusion hearing aids (amplification only) were fit to all subjects with significant hearing loss. This resulted in the greatest change in mean TFI scores in a 2-week period, from an average score of 62 to 49 (13 points). Since only one subject was an experienced hearing aid user, this improvement may reflect the immediate benefit of amplification for a new user.
Zen tones use. Zen tones were added to the subjects’ program options and they were instructed to use the Zen program daily as much as possible. On average, no significant change in TFI was measured after two weeks of Zen use (49 points to 50 points). On the other hand, we also noted that not all subjects who were instructed to use the Zen tones used them. Figure 2 shows a correlation between absolute TFI score change and hours of Zen use. A positive correlation was found between improvement in TFI and daily hours of Zen use. Indeed, the three subjects who used Zen tones more than seven hours daily had an average TFI improvement of 24 points (or 41% improvement). This suggests that tinnitus improvement on the TFI is heavily tied to actual Zen use.
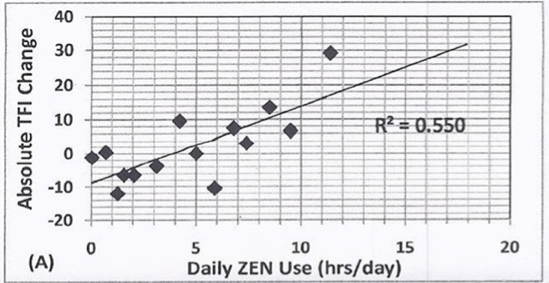
Figure 2. Scatter plot comparing absolute change in TFI scores and daily hours of use of Zen.
Adjustment based counseling (> 3 months use). Depending on the subject’s needs, this component took place in one or across several appointments. The TFI was measured 3 months later and resulted in an average further improvement of 10 points, which was a 23% change when compared to baseline. This improvement is likely due to a combination of hearing aid use, Zen use and counseling over time. The TFI score at 12 months was essentially unchanged from 6 months, indicating a sustained benefit over time.
Changes in MML and LDL
Figures 3 and 4 show the changes in MML (Figure 3) and LDL (Figure 4) between the pre- and post-training sessions. There were no significant changes in average MML or LDL measures from baseline to the end of study. The mean change in MML for all subjects was -2 dB in the right ears and -1 dB in the left ears. A significant MML change would be greater than 5 dB. Figure 4 shows the mean change in LDLs for all subjects from 1000 Hz through 4000 Hz. The mean changes ranged from +2 dB to -2 dB, also within expected clinical variability. This suggests no change in LDLs over the 12 months of the study.
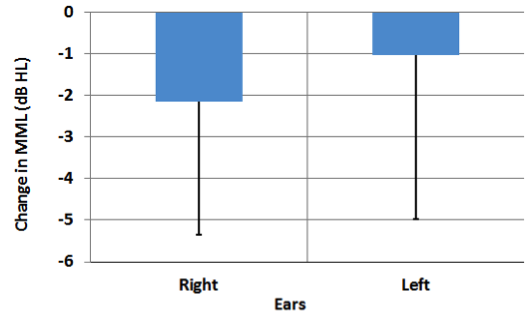
Figure 3. Changes in absolute MML between the baseline (pre-training) and end of study (post-training) sessions for the right and left ears.
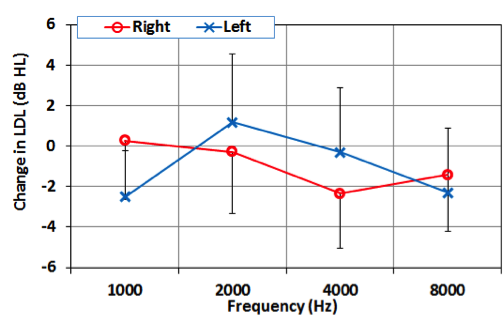
Figure 4. Mean change in LDL (dB) across frequencies between baseline and end of study sessions for the right and left ears.
Changes in VAS Ratings Over Time
Figure 5 summarize the changes in VAS ratings for each of the measured criteria. Ratings of tinnitus annoyance and awareness improved the most, by approximately 4 points on the 10 point scale (40%). The severity of tinnitus improved by approximately 20%, and the level of relaxation improved about 15%. Sensitivity to loud sounds improved only 10% on average.
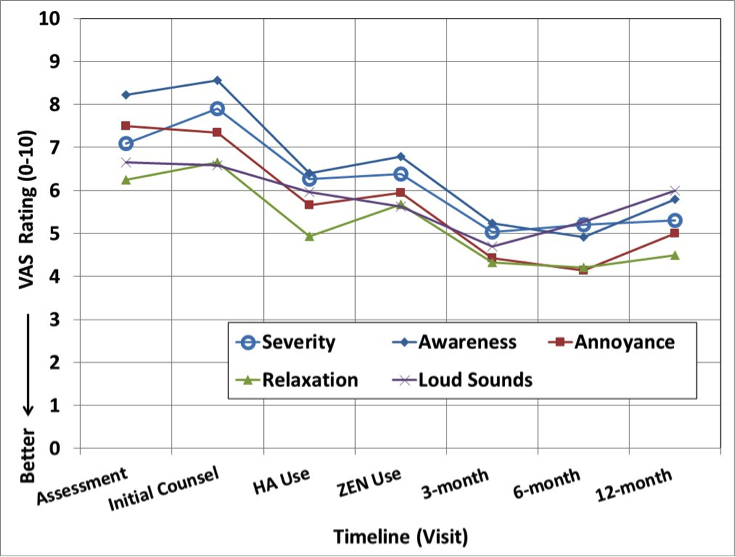
Figure 5. Changes in tinnitus ratings as measured on the visual analog scale for the five dimensions.
Data Logging
We also examined how frequently the subjects used the hearing aids and the Zen tones through the data logging capability of the hearing devices. Figure 6 summarizes the average number of hours (per day) that the hearing aid and the Zen program were used over time. It shows that use of the Zen tones was the greatest (6 hr/day) at the start of therapy and decreased over time (to < 2 hr/day). In contrast, the master or hearing aid program was used for only 4.5 hr/day initially and gradually increased to almost 7 hr/day at the end of the study.
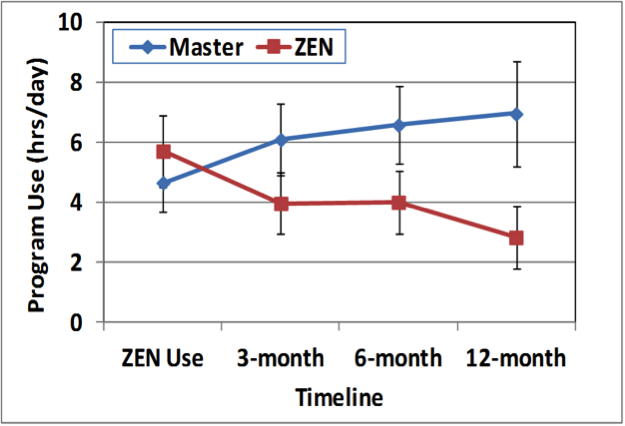
Figure 6. Program use of the hearing aid and Zen program over time.
End of Study Questionnaire
The end of study questionnaire was given at the 12 month visit to examine how much benefit subjects perceived from each component of the WZT protocol and how much overall benefit they perceived as a result of the overall WZT protocol. Figure 7 summarizes the perceived benefit of each WZT component. The following observations can be made:
- All subjects felt that the informational counseling was of benefit, even though there was no improvement shown on the TFI. Subjects likely rated this item as inclusive of all counseling components, rather than the initial informational counseling alone.
- Almost all subjects felt that hearing aid amplification was of benefit, with 73% rating the benefit as “great”.
- 67% of subjects rated the Zen tones as beneficial, with about half of those rating the benefit as “great”.
- All subjects felt that follow-up with the audiologist was of some (27%) to great (73%) benefit.
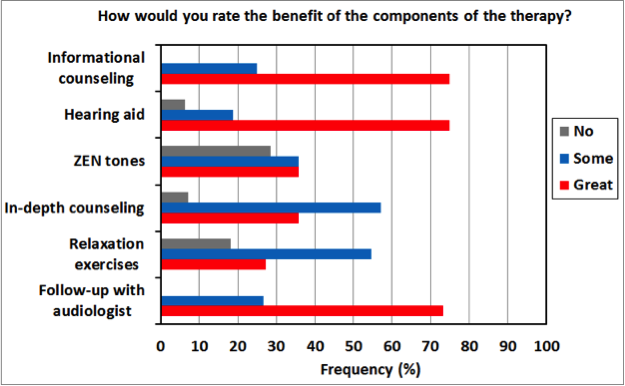
Figure 7. Frequency of perceived benefit (“no”, “some”, and “great”) for each WZT component.
Figure 8 summarizes the perceived tinnitus improvement as a result of participation in the WZT protocol. The following observations can be made:
- 83% of subjects felt that their tinnitus problem had improved “somewhat” to a “great deal”.
- Over 90% of subjects were both less distressed and less worried about their tinnitus.
- Almost 2/3 of the subjects reported sleeping better as a result of the participation.
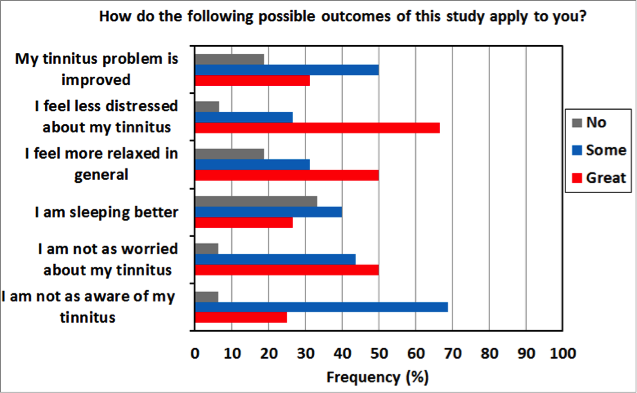
Figure 8. Areas of reported improvement as a result of participation in the WZT protocol.
Discussion
Overall, the WZT protocol was found to be effective as measured by a mean improvement in TFI scores of 28 points. This corresponds to a 45% improvement over the baseline TFI scores. The average TFI scores continued to improve up through six months, with scores generally remaining stable between the 6 and 12 month visits. This suggests a cumulative effect of the components of the WZT, and maintenance of a long-term benefit.
When considering the contribution of each component of the WZT, there was much individual variability across participants. Various components were more or less beneficial across subjects, depending on their individual needs. However, there were some general trends found in the data. The initial instructional counseling had little effect on TFI scores, suggesting that basic information on hearing loss and tinnitus alone, although educational, has little therapeutic value. Amplification resulted in the greatest benefit as measured on the TFI, reinforcing the findings of Kochkin and Tyler (2008), and possibly influenced by the fact that most subjects were first time hearing aid users. Two-thirds of the subjects reported some benefit or great benefit from Zen tones on the end of study questionnaire, in contrast to the indication of no additional benefit from hearing aid fitting to Zen fitting on total TFI score (two weeks later). It was also found that the Zen tones were used most during the first three months of therapy, possibly indicating that once the problem improved to a certain degree, Zen tones were no longer as necessary for relief. The counseling component, which included CBI, relaxation, and sleep hygiene (as needed), contributed to additional significant improvement in TFI. However, since this component took place over a longer time period (three months as compared to two weeks), it is difficult to compare to contributions of the other components. Improvement over the course of the study is likely due to a cumulative effect of multiple components of the therapy. Improvement continued through six months and then was stable through 12 months, indicating a long-term benefit from this therapy.
In contrast to the improvements seen on the TFI, VAS and end of study questionnaire, there were no significant changes found in MML or LDL measures. The MML and LDL measures are thought to be a more objective measure of changes in the auditory system related to the tinnitus perception. This underscores the difficulty of any tinnitus study to sort out changes in the emotional components of the tinnitus problem from changes in the actual tinnitus perception. Unfortunately, since we are attempting to measure a perception for which there is no direct physical correlate, we are largely dependent upon subjective questionnaires and rating scales. More research is needed to examine the correlation between self-report questionnaires such as the TFI, and psychoacoustic measures such as the MML. For now, we must be satisfied that our patients are managing better with their tinnitus, while we continue to look for methods to objectively measure, and ideally reduce, the perception.
The tinnitus problem is complicated; each patient presents a unique set of characteristics and other life factors which can contribute to the success or failure of any treatment. This needs to be recognized by the clinician and additional support provided as necessary. We found the Widex Zen Therapy to have many advantages in addressing the individual nature of tinnitus disturbance. The hearing instruments are very flexible, offering a wide range of relaxing Zen tones. In addition, white noise is available for those patients who did not like the tones or to be used in combination with the tones. The instructional counseling materials are well organized, comprehensive, but brief enough to cover in an hour or less. The additional resources provided for cognitive behavioral counseling and relaxation therapy are packaged in an easy to use format for the busy clinician who may not have had extensive training in this type of counseling. Since the inception of this study, a number of other hearing aid manufacturers have come out with similar packages of devices supported by counseling resource materials as well as smart phone applications to assist the audiologist in providing a comprehensive management program to their patients.
Appendix A
The questionnaire used by participants to rate perceived overall benefit of participation in the study and the benefit of each WZT component can be viewed here.
References
Formby, C., Sherlock, L.P., Gold, S.L., & Hawley, M.L. (2007). Adaptive recalibration of chronic auditory gain. Seminars in Hearing, 28, 295–302.
Hanley, P., & Davis, P. (2008). Treatment of tinnitus with a customized, dynamic acoustic neural stimulus: Underlying principles and clinical efficacy. Trends in Amplification, 12(3), 210–222.
Henry, J., Schechter, M., Zaugg, T., Griest, S., Jastreboff, P., Vernon, J.,...& Stewart, B. (2006). Outcomes of clinical trial: Tinnitus M=masking versus Tinnitus Retraining Therapy. Journal of the American Academy of Audiology, 17,104–132.
Henry, J.A., Stewart, B.J., Abrams, H.B., Newman, C.W., Griest, S., Martin,… Searchfield, G. (2014) Tinnitus Functional Index - development and clinical application. Audiology Today, 26(6), 40-48.
Herzfeld, M., Ciurlia-Guy, E., & Sweetow, R. (2014). Clinical trial on the effectiveness of Widex Zen Therapy. Hearing Review, 22(11).
Hoare, D.J., Searchfield, G.D., El Refaie, A. & Henry, J.A. (2014). Sound therapy for tinnitus management: Practicable options. Journal of the American Academy of Audiology, 25, 62-75.
Hobson, J., Chisholm, E., & El Refaie, A. (2012). Sound therapy (masking) in the management of tinnitus in adults. Cochrane Database of Systematic Reviews, Issue 11. Art. No.: CD006371. DOI: 10.1002/14651858.CD006371.pub3.
Jastreboff, P.J. & Hazell, J.W.P. (1998). Treatment of tinnitus based on a neurophysiological model. In J. Vernon (Ed.), Tinnitus: treatment and relief, (pp. 201-216). Boston, MA: Allyn & Bacon.
Johansen, J.D., Skellgaard, P.H., & Caporali, S. (2014). Effect of counseling, amplification and fractal tones in tinnitus management. Communication Disorders, Deaf Studies and Hearing Aids, 2, 124. doi:10.4172/2375-4427.1000124
Kochkin, S., & Tyler, R. (2008). Tinnitus treatment and the effectiveness of hearing aids: Hearing care professional perceptions. Hearing Review, 15, 14-18.
Kuk, F., & Peders, H. (2008). Hearing aid as a music synthesizer. Hearing Review, 15, 28-38.
Lockwood, A., Salvi, R., & Burkard, R. (2002). Tinnitus. New England Journal of Medicine, 347(12),904-910.
Martinez-Devesa, P., Perera, R., Theodoulou, M., & Waddell, A. (2010). Cognitive behavioural therapy for tinnitus. Cochrane Database of Systematic Reviews, Issue 9. Art. No.: CD005233. DOI: 10.1002/14651858.CD005233.pub3
Meikle, M.B. (1997). Electronic access to tinnitus data: The Oregon Tinnitus Data Archive. Otolaryngology- Head and Neck Surgery, 117, 698–700.
Meikle, M. B., Henry, J. A., Griest, S. E., Stewart, B. J., Abrams, H. B., McArdle, R.,… Vernon, J. A. (2012). The Tinnitus Functional Index: Development of a new clinical measure for chronic, intrusive tinnitus. Ear and Hearing, 33,153–176.
Sedley, W., Gander, P., Kumar, S., Oya, H., Kovach, C., Nourski, K., …Griffiths, T. (2015). Intracranial mapping of a cortical tinnitus system using residual inhibition. Current Biology, 25(9),1208 -1214.
Sweetow, R., Kuk, F., & Caporali, S. (2015). A controlled study on the effectiveness of fractal tones on subjects with minimal need for amplification. Hearing Review, 22(9), 30.
Sweetow, R., & Sabes, J. H. (2010). Effects of acoustic stimuli delivered through hearing aids on tinnitus. Journal of the American Academy of Audiology, 21, 461-473.
Tyler, R.S., & Baker, L.J. (1983) Difficulties experienced by tinnitus sufferers. Journal of Speech and Hearing Disorders, 48(2),150-154.
Yetiser, S., Tosun, F., Satar, B., Arslanhan, M., Akcam, T., & Ozkaptan, Y. (2002). The role of zinc in management of tinnitus. Auris Nasus Larynx, 29, 329-333.
Citation
Stocking, C.T., & Stecker, N.A. (2016, December). Efficacy of the individual components of a tinnitus management protocol. AudiologyOnline, Article 18326. Retrieved from https://www.audiologyonline.com.


