
Learning Outcomes
After this course learners will be able to:
- Describe the main effects of vented and open fittings during hearing aid verification.
- Describe the clinical purposes of simulated real ear measurement (S-REM) and how it relates to preferred practice and remote practice.
- Recognize the key elements of a new venting correction feature applied to test box hearing aid verification.
Introduction
Real-ear measurement (REM) has long been recognized as best practice for the fitting and verification of hearing instruments to ensure proper performance and increase the likelihood of patient benefit (AAA, 2006).
Simulated REM (S-REM) via test box measurements was developed to offer another method of verification in cases where it was not possible or desirable to conduct standard REM (Seewald et al., 1999). Examples of this use of S-REM include pediatric populations, difficult to test patients, and adult pre-fitting. Recent best practice guidelines include this verification option especially for children (AAA, 2013) and enhancements to S-REM now include the prediction of earmold real-ear to coupler differences (RECDs) from foam tip RECDs (Moodie et al., 2016).
Beyond the historical drivers that led to the development of S-REM, the current global pandemic has created increased demand for minimal contact procedures in clinical practice. Given the proximity required between patient and provider during REM, some clinics have adopted the use of S-REM with a wider range of patient types, including adults, to facilitate remote fitting and drop-off / drop-box service delivery.
While S-REM is a validated predictor of actual on-ear performance, particularly in cases where the individual patient’s RECD is measured (see review in Bagatto et al., 2005), challenges with capturing vent effects in the occluded conditions of the test box have remained, particularly in cases with significant venting. This reality has led to an inability to accurately simulate real-ear measurements in the test box with open fittings - until now.
With the introduction of software versions 4.24 (Verifit2) and 1.30 (Axiom), Audioscan is now providing clinicians with the option of selecting from a range of venting options when verifying in the test box mode. The venting corrections within Speechmap® will apply an acoustic correction that considers the combined impact of two components: direct vent-transmitted sound that enters the vent and passes through to the ear canal, and amplified sound from the hearing aid that exits the vent. This correction was developed to improve the prediction of the overall dB SPL level at the eardrum when coupler-based measures are used. While REM is the gold standard for hearing aid verification, this new simulated venting feature provides additional improvement in the estimated dB SPL levels in cases where REM is not possible.
Open Versus Vented Hearing Aids
Modern hearing instruments offer a wide range of venting options and configurations. Among these possibilities, open fittings are often chosen during the selection and fitting of hearing instruments. Open fittings can be provided using multiple earpiece coupling techniques. Commonly, this venting configuration is offered in products fitted using instant-fit non-custom domes or sleeves that are highly vented, often by placing perforations in the material itself. Open-fit products may take the form of slim tube fittings or devices that place the receiver in the ear canal (e.g., RICs). Both of these open-fit product types can also be fitted with custom-molded sleeves or earpieces rather than pre-made domes with a range of venting configurations. For instance, either the sleeves or domes may also be semi-open or closed as desired. Closed or semi-closed fittings are commonly thought of as being produced by sleeves or domes that have few or no vent holes, however as with any coupling type, the size of the ear canal can also impact the functional venting effect. For example, if the vent holes in the dome are pinched shut in a small ear canal, the actual vent effect may be less than anticipated. Conversely, a closed dome may in fact be somewhat open if it does not fully occlude the canal due to the effects of slit leaks around the edges of the dome or the sound absorption of the material. For these reasons, the exact degree of openness in any instant-fit dome or sleeve-based fitting is individualized. Further details on open fittings can be found in Winkler et al., 2016.
In contrast to open fittings, vented fittings are commonly understood to be provided using custom-molded products, either in the ear or with an earmold coupled to a BTE hearing aid. That said, custom earpieces can provide an ‘open fitting effect’ if a large enough vent is created during manufacturing. In these cases, the vent is commonly a physical hole that is drilled through the custom earpiece which can vary in diameter and length throughout.
Regardless of the venting method chosen, open and vented products are commonly designed to allow: (1) airflow into and out of the ear; (2) release of pressure during earpiece removal and/or insertion; (3) flow of sound into and out of the vent. The third component (sound flow into and out of the vent) has been of particular interest in the fitting and verification of hearing instruments given the challenges of appropriately accounting for vent effects, particularly during test box-based measurement procedures. To properly address these venting issues with a range of coupling options and configurations across product types, we have developed a simulated venting correction and associated protocol. This protocol proposes a series of steps that evaluate the third aspect (sound flow into and out of the vent) for either vented or open products. Because both product categories can have no venting effect, a small venting effect, or a large venting effect, the same protocol can apply to both.
The Acoustic Effects Of Vents And Open Tips
The venting effects of various instant-fit dome styles, coupling options and custom earpieces are well- described (Blau et al., 2008; Caporali et al., 2019; Winther et al., 2020; Winkler et al., 2016, Kuk & Keenan, 2006; Zachman & Studebaker, 1970). As a rule, the larger the vent, the greater the venting effect. This is true whether the fitting uses a single, large diameter vent, or is the result of the sum of several smaller vents. The length of the vent also plays a significant role (Kuk et al., 2009), with shorter vents typically resulting in a greater venting effect than a longer vent for the same vent diameter. The combined effects of vent diameter, shape, and length can be summarized in to a single value that quantifies the acoustic mass of the vent (Vogl & Blau, 2019). For example, several small vent holes distributed around a non-custom dome may sum to produce a large venting effect overall. Similarly, a small, drilled vent in a custom product combined with slit leak vents around the outside of the earpiece due to poor fit may combine to produce a large venting effect.
Large versus small venting effects usually can be differentiated by the frequency range they affect. A large vent allows a flow of sound in through the vent and out from the vent over a broader range of frequencies than is allowed through a small vent. This effect of venting starts at the very low frequencies and expands upwards in frequency as the size of the vent is increased. Large venting effects, as would typically occur in an open fitting, are usually desirable when the listener has normal or near-normal hearing in the low frequencies. Provision of acoustic, rather than aided, sound via vent transmission may preserve the normal low frequency cues that are used for horizontal sound localization and pitch perception. In addition, a vent may allow the exchange of air into and out of the ear canal. Overall, these effects may support a more natural sound quality and intelligibility (Cox & Alexander, 1983), spatial hearing (Keidser et al., 2007; Noble et al., 1998), and avoid creation of an anaerobic environment in the external ear canal.
How Can I Verify Vented Or Open Fittings?
Three main considerations in the assessment of vented and open fittings include: (1) How much sound is coming in through the vent? (2) Is the listener’s own voice being occluded by the ear-worn device? (3) Is the overall fitting (vent-transmitted plus aid-transmitted sound) providing an appropriate fitting? Historically, given challenges with accounting for vent-effects in the occluded conditions of the test box, open fittings have been verified on the ear of the patient (e.g., via REM). The protocols for on-ear verification of open fittings are well-established and are typically focused on ensuring that vented amplified sound does not contaminate the sound field calibration routine by being received by an active reference microphone outside the ear canal. As such, verification system manufacturers typically provide an on-ear ‘Open’ vent setting which guides the fitter through a stored equalization calibration routine (Figure 1). For a detailed discussion of REM verification considerations with open fittings, see Mueller & Ricketts, 2006 and Pumford, 2018.
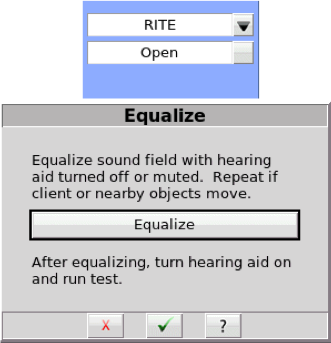
Figure 1. Example of a stored modified pressure method equalization prompt from one manufacturer upon beginning REM with an open fitting.
How Can I Measure Fit-to-Targets for Vented Fittings?
As discussed above, the gold standard for fitting to targets and assessing speech audibility is to measure hearing instruments using REM. This verification technique considers the combined effects of vent- transmitted and hearing-aid-transmitted sound on the overall signal level received at the eardrum of the patient. Together, these factors provide access to a broad bandwidth of speech, with the low frequencies typically the result of vent-transmitted sound, the mid- frequencies a blend of vent and hearing-aid transmitted sound, and the high frequencies mainly from the hearing aid. The hearing-aid-dominated region will be adjustable with hearing aid software, while the vent- transmitted region will be influenced by modifications to the degree of venting or occlusion in the earpiece (Figure 2).
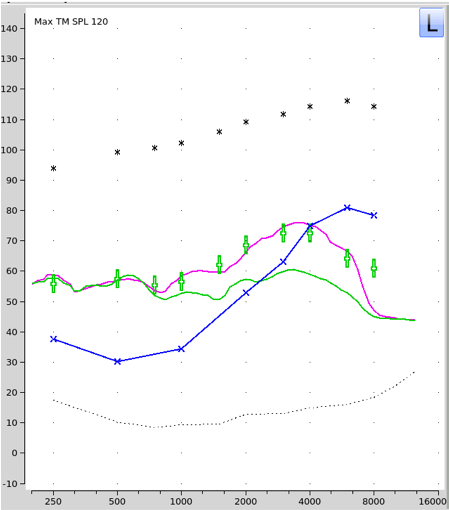
Figure 2. REM of an open fitting showing vent- transmitted signal (green curve) with hearing aid off (i.e., real-ear occluded response), and aid- transmitted signal (purple curve) with hearing aid on (i.e., real-ear aided response).
What if I Can't Do REM with My Patient?
If REM is not possible, we often turn to simulated real ear measurement (S-REM). Traditionally, this approach has been developed and validated for use with young children who typically have had minimally vented or occluded earmolds (Moodie et al., 1994), and recently updated to include corrections for the differences between foam tips and earmolds (Moodie, et al., 2016; Scollie, 2016). However, S-REM and its applications have not historically accounted for the effects of venting. Some prescriptive targets include corrections for venting in the development of coupler targets for verification, accounting for both sound entering the ear canal through the vent and sound exiting the ear canal through the vent in a two-stage process (Bagatto et al., 2005). However, the real-ear aided response (REAR) targets do not vary as a function of vent selection: the displayed prescriptive targets can be met by sound pressure levels present in the ear canal from the combination of vent-transmitted and hearing-aid- transmitted sound. To keep a consistent display with REM mode, test box measures and associated targets in test box Speechmap with Audioscan systems are also displayed in REAR format and are transformed to dB SPL levels at the eardrum (i.e., S-REM). As a result, users will note that the REAR targets in test box Speechmap do not vary as a function of vent selection. However, as will be described, venting transforms can now be applied to the measured coupler response based on the coupling and vent combination selected in Speechmap. Prior to a recent software update, venting corrections have not been a part of the S-REM transformation process.
Thus, to improve S-REM, a new two-stage process has been developed that accounts for two sound paths associated with venting: (1) unaided sound coming into the ear canal through the vent, and (2) aided sound exiting the ear canal through the vent. This software development allows professionals to apply venting corrections to the measured levels from the hearing aid when verifying within the test box. The corrections were designed to improve the accuracy of S-REM predictions with open and vented products, so that they are more representative of on-ear performance.
Using this option requires that the professional enters the on-ear coupling type and associated venting style in a new menu, so that the appropriate venting effects can be applied.
How does the Simulated Venting Correction Work?
In test box Speechmap, the effects of a vented fitting are applied according to the coupling and venting of the selected hearing instrument (Figure 3). The vent correction has two components: (1) the effect of unaided sound entering the ear canal through the vent (bypassing the hearing instrument) from the sound source, and (2) the effect of aided sound leaking out of the ear, through the vent. The values used were derived from published studies (Blau et al., 2008; Caporali et al., 2019; Kuk & Keenan, 2006; Zachman & Studebaker, 1970). A transform of the unaided sound reaching the tympanic membrane (TM) through the vent is combined with the measured coupler SPL modified by the effect of sound leaking out of the ear through the vent to produce a vented S-REM output that includes the predicted vent effects from the correction. As with all S-REMs, the predicted ear canal SPL will also include microphone location effects (MLEs) and RECDs, using the same procedures that have been used previously (Bagatto et al., 2005; Moodie et al., 2016; Scollie, 2016).
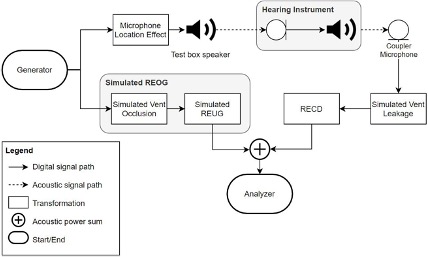
Figure 3. Simulated venting correction for test box verification. The simulation consists of two branches: one for aid-transmitted sound and one for vent-transmitted sound. Both branches are combined (power sum) to account for venting in simulated REM.
Vent Correction Part 1: Simulated Vent-Leakage Component
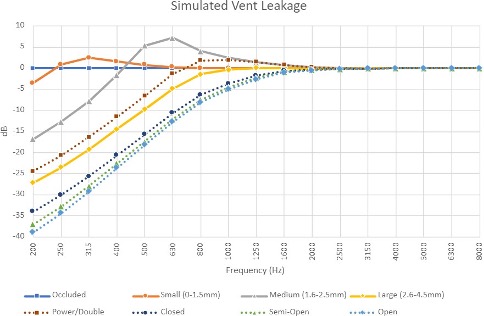
The simulated vent- leakage is applied to the measured coupler signal and represents the effect of the fitting on the hearing instrument output in the ear canal. Per Figure 4, this transform affects the frequency range from ~200 to 3150 Hz, with the majority of the effect below about 800 Hz. Based on availability of data in the high frequency region, the vent effect on aid-transmitted sound above 3150 Hz is designed to converge to zero, resulting in no changes to the measured coupler signal. Small Helmholtz resonances are observed at frequencies just above the main vent loss range for most dome styles; this effect decreases as the degree of occlusion increases. The transform is applied to the aided sound path, so a value of -10 dB would act to reduce the displayed S-REM levels. The impact of this vent correction component on the final measured output depends on the relative levels of amplified versus unamplified sound and which one is dominant. The RECD is subsequently applied to the coupler measurement. Per typical protocols, the RECD data does not include venting and reflects real- ear measures gathered in an occluded state. Venting considerations are captured elsewhere outside of the RECD transform as highlighted in Figure 3.
Vent Correction Part 2: Simulated Vent- Transmitted Component / REOG
In addition to the simulated vent-leakage component outlined above, a simulated vent-transmitted component is combined with the simulated aid- transmitted (amplified) sound component. In this part of the venting correction, unaided sound is expected to travel into the ear canal through the vent. Sound will enter across a broader range of frequencies as the vent size is increased. The vent-transmitted sound levels at the tympanic membrane are estimated using simulated real-ear occluded gain (REOG: Figure 5) specific to each vent type. In all cases, the REOG reflects the combination of a simulated vent-specific occlusion factor and simulated adult average real-ear unaided gain (REUG). The simulated vent-transmitted / REOG component illustrates that most hearing aid couplings are expected to have sound transmission in through the vent to approximately 1000 Hz, with open styles extending above this frequency to the 4000 Hz region. Further, it can be observed that as the hearing aid coupling becomes more open, it becomes more likely that a residual external ear canal resonance will be observed as part of the correction. This sound transmission pattern agrees with tutorials and clinical examples of the venting effects associated with open fittings (Kuk & Keenan, 2006; Mueller & Ricketts, 2006; Winkler et al., 2016). As noted with the vent-leakage component, the extent to which the vent-transmission component will impact S-REM is dependent on which sound path (i.e., amplified versus unamplified) is dominant. As the amplified signal becomes progressively greater relative to the unamplified path, the impact of the vent correction is lessened to reflect what would occur during REM.
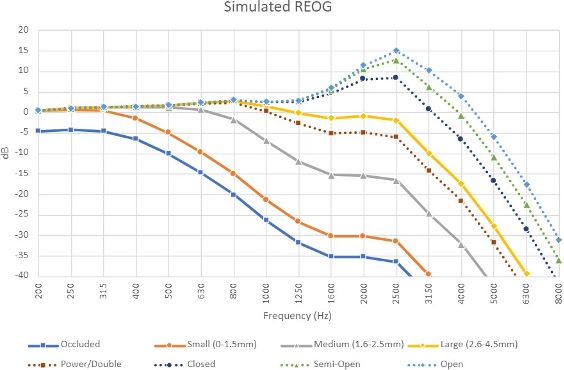
Figure 5. Estimated Real Ear Occluded Gain (REOG) transforms for 4 custom earpiece couplings (solid lines) and 4 instant-fit couplings (dashed lines).
Clinical Impact of Simulated Venting in S-REM
In summary, the main purpose of the vent correction is to improve the accuracy of S-REM for vented fittings in the occluded measurement conditions of the test box. Vent-associated error in S-REM may be observed in two ways: (1) if the fitting requires little or no gain in the low frequencies, the on-ear fitting will likely have good low-frequency audibility from vent-transmitted sound but the test box fitting may look under target in the low frequencies if vent transmission is not included; (2) if the fitting requires gain in the low frequencies but also uses some venting, the fitting may be on target for REM, but over target in the test box for the low frequencies. This error occurs because some of the aided sound is leaking out of the ear canal when worn but is retained in the sealed coupler. For both cases, an effective vent correction should improve the accuracy of S-REM.
The effects of the venting choices in Speechmap are illustrated in Figure 6 for different dome types relative to an occluded custom earmold. The displayed measurement curves are unaided, so they illustrate the expected sound transmission path for unaided sound traveling in through the vent. Figure 6 clearly illustrates that the S-REM prediction expects a greater level of unaided sound to enter the ear canal as the dome type is more open.
Similar transforms are used for vent sizes in custom earmolds, with choices including occluded, small, medium, large, and open. Millimeter ranges associated with each vent size are provided in the menu for reference (Figure 7). Just as was observed for the dome styles, the vented S-REM will build in a greater frequency range of unaided sound transmission for larger vents with custom earpieces.
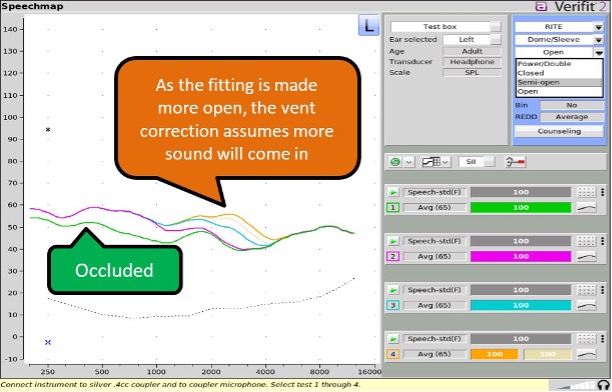
Figure 6. Dome/Sleeve comparison. Test 1 (green) = mold, occluded; Test 2 (purple) = power/double dome; Test 3 (blue)= closed dome; Test 4 (shaded dotted line) = semi-open dome; Test 4 (orange) = open dome.
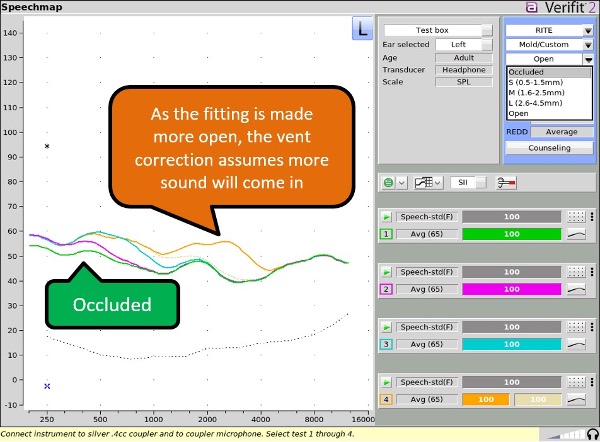
Figure 7. Mold/Custom comparison. Test 1 (green) = mold, occluded; Test 2 (purple) = small vent (0.5-1.5mm); Test 3 (blue) = medium vent (1.6-2.5mm); Test 4 (shaded dotted line) = large vent (2.6-4.5mm); Test 4 (orange) = open vent.
How to Use Simulated Venting S-REM in the Test Box
S-REM conducted using the simulated venting corrections is very similar procedurally as S-REM prior to the correction. For instance, hearing instruments are still connected to couplers using the same hardware and procedures and RECD measures are still recommended if possible. In addition to choosing from previously existing audiometric items (e.g., fitting formula, transducer, etc.) and hearing instrument types, clinicians will now have access to two new dropdown menus that allow for selection of hearing instrument on-ear coupling and associated vent type.
What are the Coupling and Venting Options?
The new vent simulation considers the most commonly used coupling types and venting sizes from the major hearing instrument manufacturers. Categorization was developed first in terms of the on-ear coupling type, followed by the associated venting options assuming an average vent length. A breakdown of the available options in a recent software release is illustrated in Figure 8. To apply the venting correction in S-REM, simply select the coupling and associated venting option that most closely represents the on-ear venting characteristics of the product you are fitting. If desired, ‘disable’ the simulated venting feature and obtain S-REM results equivalent to previous software versions by selecting ‘None’ from the vent selection drop-down menu.
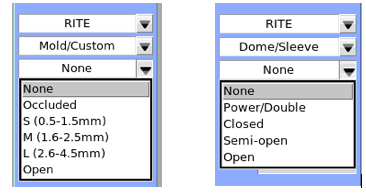
Figure 8. Coupling and Venting Options in test box Speechmap. Note that “None” disables the vent correction feature.
Applying the Simulated Venting Corrections in Speechmap: Effect Examples
The overall size and frequency range of the applied vent correction will vary depending on the test level, the gain of the hearing aid, and the coupling/venting option selected. For illustration, consider the two simulated cases in Figure 9, each fitted with a custom earpiece or ear mold with either the open (solid colored lines) or the occluded (dashed colored lines) vent corrections applied. In each case, the hearing aid settings remained constant for all measures. As such, any change in device output reflects the application of the vent correction and provides a general indication of the effect that could be observed using similar device settings and measurement variables. The top panel shows a case with a mild sloping to moderate sensorineural hearing loss (SNHL). The impact of the vent correction from occluded to open in this case is fairly small given minimal low to mid frequency gain. We can note the impact of vent-transmitted sound in the low frequencies with the simulated REM open fitting (which would benefit from vent-transmitted sound during actual REM) being higher than the occluded condition where minimal vent-transmitted sound would be present. We can also note differences in the simulated REM in the mid-frequency region where an actual REM response would reveal mixing between the vent-transmitted and amplified sound paths in an open fitting versus an occluded state. The bottom panel shows an example case with a mild sloping to severe SNHL where the hearing aid gain is relatively higher than the previous example. In this case, note that the simulated REM open fitting reveals the impact of anticipated venting of the low frequency gain, resulting in a predicted REM in the low frequencies that is equivalent to the earlier example in the top panel. Essentially, we are seeing the direct vent- transmitted path in the simulated open condition in the low frequencies, whereas the simulated occluded vent condition shows a relatively higher response in the low to mid frequencies as the amplified sound path would not be vented. As there is more gain at lower input levels than louder input levels, the difference between the open and occluded fittings is relatively greater at lower input levels than louder input levels in this case.
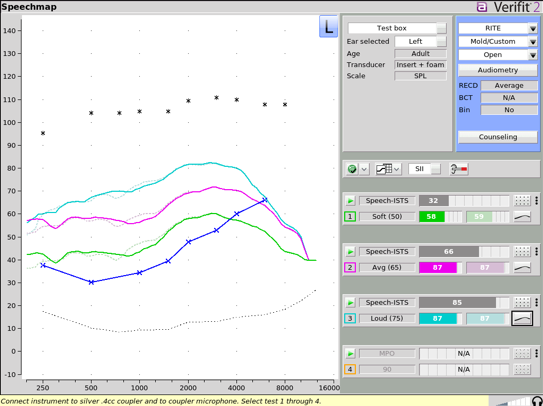
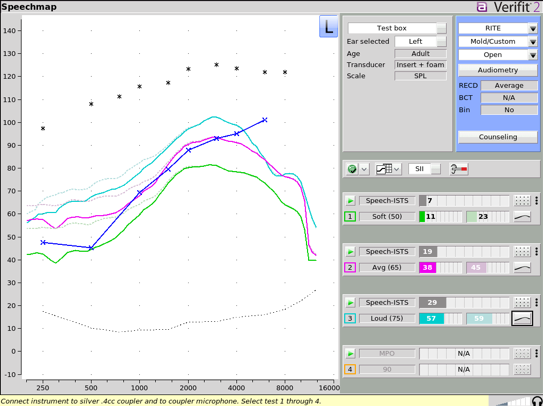
Figure 9. Comparison of two simulated cases with either open (solid colored lines) or occluded (dashed colored lines) venting menu settings. Results are shown for soft (green curves), average (purple curves) and loud (blue curves) speech. Differences between the solid and dashed lines for each input level are due to the venting correction in S-REM (i.e., hearing aid programming was held constant).
Applying the Simulated Venting Corrections in Speechmap: Real Case Examples
The effects of the simulated venting correction can also be illustrated with the two following patients who had hearing aids that were verified and fine-tuned to target with REM. We also verified each hearing aid using traditional S-REM without venting corrections, and with the new simulated venting S-REM options. Individually measured foam tip RECDs were used in all conditions for both patients.
Case 1: Normal low-frequency hearing and significant venting with little low-frequency gain
This hearing aid user was fitted to DSLv5-adult prescriptive targets using REM and an open dome on a receiver-in-the-canal (RIC) hearing aid style (Figure 10). This hearing aid user has mild hearing loss with good access to unaided sound in the low-to-mid frequencies, so one of the fitting goals was to provide a significant amount of venting. The combined vent transmitted and hearing-aid-amplified sound are shown together in the REM for inputs of 55, 65, and 75 dB SPL speech, along with an MPO signal. Testing revealed a good fit to targets (top left panel).
The slight over-target response at 250 Hz is likely attributable to vent-transmitted unaided sound. The hearing aid was re-verified in a sealed coupler using test box measures without vent corrections (top right panel) using the same input signals as with the REM condition. The S-REM measure without a venting correction shows an under-target response in the mid-frequencies because the combined effects of the unamplified vent-transmitted sound and the simulated vent-leakage component with an open dome are not present in this measurement. When the simulated venting correction is applied (per menu in bottom left panel) the vent-transmission and vent-leakage components typical of an open fitting are included in the measurement resulting in an improved prediction of the user’s actual REM (bottom right panel).
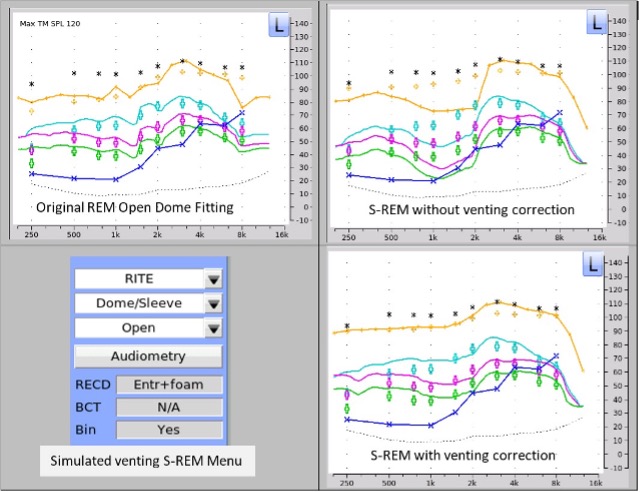
Figure 10. Case illustration of REM versus simulated REM with and without venting corrections for 55, 65, and 75 dB SPL speech and the MPO signal. This case used an open dome and little low-frequency gain.
Case 2: A mild to moderately severe gently sloping loss with venting and low-frequency gain
This older adult was fitted to the DSLv5-adult hearing aid prescription using REM (Figure 11). The original fitting was completed with a RIC hearing aid and a closed dome for inputs of 55, 65, and 75 dB SPL speech, along with an MPO signal. The fitting shows a close match to targets (top left panel). The hearing aid was re-verified in a sealed coupler using test box measures without vent corrections (top right panel) using the same input signals as with the REM condition.
This measure shows an over-target response in the low frequencies primarily attributable to the lack of a vent-leakage component in this measurement. When the simulated venting correction is applied (per menu in bottom left panel) the vent-leakage component results in a decrease in the measured response and an improved prediction of the user’s actual REM (bottom right panel).
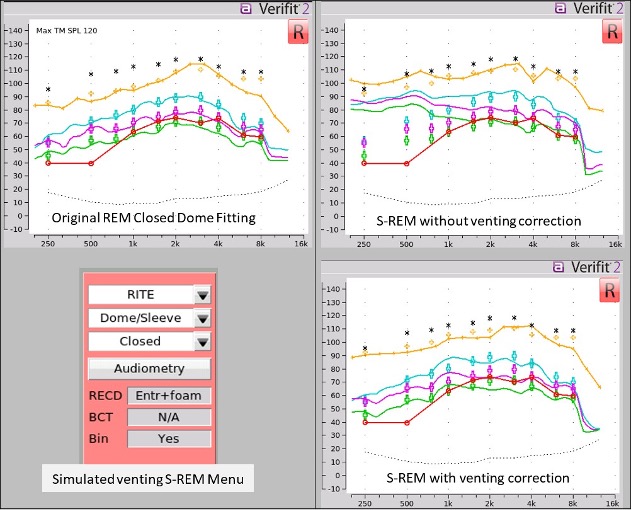
Figure 11. Case illustration of REM versus simulated REM with and without venting corrections for 55, 65, and 75 dB SPL speech and the MPO signal.. This case used a closed dome and gain in the low frequencies.
Summary
A new venting correction has been added to the simulated real ear measurement (S-REM) function, which is found within Speechmap when test box verification is selected. This new venting correction provides support for the verification of vented and open fittings, with the goal of improved accuracy in S-REM predictions of REM versus previous software versions that did not account for venting effects. Although REM is still considered the gold standard for verification of hearing aids, REM is not always possible. S-REM was originally developed as a REM alternative for use with infants and young children (Seewald, et al., 1999), but can also provide a verification solution for pre-fitting and remote or low-contact hearing aid fitting and verification for hearing aid users of all ages. With the increasing use of vented and open fittings, enhancement of S-REM to include simulated venting has widespread clinical application. Recent software (Verifit2 version 4.24 and later; Axiom version 1.30 and later) now provides simulated venting corrections for test box Speechmap. The simulated venting corrections have been validated on a sample of adults wearing hearing aid styles that included BTE, receiver-in-canal (RIC), and in-the-ear (ITE) devices, across a wide range of hearing losses. This validation study is in preparation for publication and indicates significant improvement in S-REM prediction of REM, as shown in Scollie et al. (2021) and the illustrative case studies above.
References
American Academy of Audiology. (2006). Guidelines for the audiologic management of adult hearing impairment. Retrieved from https://audiology-web.s3.amazonaws.com/migrated/haguidelines.pdf_53994876e92e42.70908344.pdf
American Academy of Audiology (2013). American Academy of Audiology clinical practice guidelines on pediatric amplification. Retrieved from https://www.audiology.org/sites/default/files/ publications/PediatricAmplificationGuidelines.pdf
Bagatto, M., Moodie, S., Scollie, S., Seewald, R., Moodie, S., Pumford, J., & Liu, K. P. R. (2005). Clinical protocols for hearing instrument fitting in the desired sensation level method. Trends in Amplification, 9(4). https://doi.org/10.1177/108471380500900404
Blau, M., Sankowsky, T., Stirnemann, A., Oberdanner, H., & Schmitt, N. (2008). Acoustics of open fittings. The Journal of the Acoustical Society of America, 123(5), 3011–3011. https://doi. org/10.1121/1.2932603
Caporali, S. A., Cubick, J., Catic, J., Damsgaard, A., & Schmidt., E. (2019). The vent effect in instant ear tips and its impact on the fitting of modern hearing aids. Proceedings of the InternationalSymposium on Auditory and Audiological Research. Vol. 7. Retrieved from https://proceedings. isaar.eu/index.php/isaarproc/article/view/2019-25/378
Cox, R. M. & Alexander, G.C. (1983). Acoustic versus electronic modifications of hearing aid low- frequency output. Ear and Hearing; 4(4):190-196. https://doi.org/10.1097/00003446-198307000- 00003
Keidser, G., Carter, L., Chalupper, J., & Dillon, H. (2007). Effect of low-frequency gain and venting effects on the benefit derived from directionality and noise reduction in hearing aids. International Journal of Audiology, 46(10), 554–568. https://doi.org/10.1080/14992020701481698
Kuk, F., Keenan, D., & Lau, C. (2009). Comparison of vent effects between a solid earmold and a hollow earmold. Journal of the American Academy of Audiology, 20(8), 480–491. https://doi. org/10.3766/jaaa.20.8.3
Kuk, F., & Keenan, D. (2006). Fitting tips: How do vents affect hearing aid performance? Hearing Review, 13.2:34.
Moodie, K. S., Seewald, R. C., & Sinclair, S. T. (1994). Procedure for predicting real-ear hearing aid Performance in Young Children. American Journal of Audiology. 3(1): 23-31. https://doi. org/10.1044/1059-0889.0301.23
Moodie, S., Pietrobon, J., Rall, E., Lindley, G., Eiten, L., Gordey, D., …& Scollie, S. (2016). Using the real- ear-to-coupler difference within the American Academy of Audiology pediatric amplification guideline: Protocols for applying and predicting earmold RECDs. Journal of the American Academy of Audiology, 27(3). https://doi.org/10.3766/jaaa.15086
Mueller, H. G., & Ricketts, T. A. (2006). Open-canal fittings. Ten take-home tips. The Hearing Journal, 59(11), 24.26,28-32,34,36-39 https://doi.org/10.1097/01.HJ.0000286216.61469.eb
Noble, W., Sinclair, S., & Byrnet, D. (1998). Improvement in aided sound localization with open earmolds: Observations in people with high-frequency hearing loss. Journal of the American Academy of Audiology, 9(1), 10.
Pumford, J. (2018). Considerations in real-ear measurement: Points to Ponder. Canadian audiologist. 5(3). Retrieved from https://www.canadianaudiologist.ca/issue/volume-5-issue-3-2018/real-ear- measurement-feature/
Scollie, S. (2016). New RECDs and a New ANSI standard: Revisiting RECD basics and applications. AudiologyOnline. Article 16380. Retrieved from https://www.audiologyonline.com/articles/new- recds-and-ansi-standard-16380
Scollie, S., Pumford, J., Folkeard, P., Pietrobon, J., & Abbasalipour, P. (2021, March). Test Box Verification of Vented Fittings: Development and First-stage Validation. Poster presented at the Phonak Sound Foundation Through Early Amplification Conference. https://docs.audioscan.com/library/ posters/2021_vented_srem.pdf
Seewald, R. C., Moodie, K. S., Sinclair, S. T., & Scollie, S. D. (1999). Predictive validity of a procedure for pediatric hearing instrument fitting. American Journal of Audiology, 8(2). https://doi. org/10.1044/1059-0889(1999/017)
Vogl, S., & Blau, M. (2019). Individualized prediction of the sound pressure at the eardrum for an earpiece with integrated receivers and microphones. The Journal of the Acoustical Society of America, 145(2), 917–930. https://doi.org/10.1121/1.5089219
Winkler, A., Latzel, M., & Holube, I. (2016). Open versus closed hearing-aid fittings: A literature review of both fitting approaches. Trends in Hearing, 20, 233121651663174. https://doi. org/10.1177/2331216516631741
Winther, B., Townend, O., Stiefenhofer, G., & Switalski, W. (2020). Reducing hearing aid delay for optimal sound quality: A new paradigm in processing. Hearing Review. 2020;27(4):20-26
Zachman, T. A. & Studebaker, G. A. (1970). Investigation of the acoustics of earmold vents. The Journal of the Acoustical Society of America, 47(4B), 1107–1115. https://doi.org/10.1121/1.1912012
Citation
Pumford, J., Scollie, S., Folkeard, P., Pietrobon, J., Abbasalipour, P. (2021). Vent corrections for simulated real-ear measurements of hearing aid fittings in the test box. AudiologyOnline, Article 27884. Retrieved from https://www.audiologyonline.com





