
 From the Desk of Gus Mueller
From the Desk of Gus Mueller

It was back in the mid-60s, thanks to the work of Harry Teder, Earl Harford and others, that we first heard about this special type of hearing aid, designed to transfer a signal from the side of the head where hearing was unaidable, to the other ear, where hearing was normal, or at the least aidable. Appropriately, this hearing aid was called the Contralateral Routing of Signals, or CROS, and was soon joined by a companion product, termed a bilateral CROS, or BiCROS. At the time, the most efficient way to accomplish the ear-to-ear transfer was to embed a wire in the frame of an eyeglass hearing aid.
Both audiologists and manufacturers became quite intrigued by this new fitting approach, and in Michael Pollack’s 1975 hearing aid text, you will find a review of the various CROS modifications, including the MINI-CROS, FOCAL-CROS, HIGH-CROS, UNI-CROS, MULTI-CROS, IROS, FROS, and yes, you guessed it, the CRIS-CROS. As time went on, however, interest in CROS hearing aids faded. One exception was Telex’s introduction of a wireless (FM) BTE version, which dominated the market for many years—so much so that many companies didn’t even offer a CROS product. In general, the CROS hearing aid tended to become known as a product that wasn’t very pretty, with few features, with limited control of gain and output. Not really expected to provide optimum benefit.
But things have changed, and in a big way. Today, CROS hearing aids, more or less, have all the special features and programming capabilities that we would expect to find with the top-of-the-line premier RIC products. Because many currently available hearing aids, when fitted bilaterally, are equipped with ear-to-ear wireless full-audio sharing of data, the processing needed for CROS already is readily available. CROS or BiCROS, therefore, really has become a programmable fitting application, rather than a hearing aid per se. So, with all these great features and the programming flexibility of the modern CROS and BiCROS systems, do we maybe need to rethink the potential benefit of these fitting applications for our patients? We’ll find out in this month’s 20Q.
Erin Picou, AuD, PhD, is Assistant Professor, Hearing and Speech Science, Vanderbilt University Medical Center in Nashville. She also is the Director of the Hearing and Affect Perception Interest Laboratory at Vanderbilt, and she teaches and mentors AuD and PhD students. She currently is an Editor in the area of amplification for both the American Journal of Audiology and Ear and Hearing, and in the past year, was named the outstanding reviewer for the International Journal of Audiology. Dr. Picou also serves on the hearing aid standards committee of the Audiology Practice Standards Organization.
If you’ve taken a look at the contents of an audiology journal anytime in recent years, you no doubt have seen Erin’s name as an author on one of the articles. I suspect she is one of audiology’s most prolific researchers and writers. And importantly, not only is her research well-designed and scientifically sound, in many cases, there are direct clinical applications. You will see this first hand in this month’s 20Q.
Gus Mueller, PhD
Contributing Editor
Browse the complete collection of 20Q with Gus Mueller CEU articles at www.audiologyonline.com/20Q
20Q: Amplification Options for Unilateral Hearing Loss - A Case for CROS
Learning Outcomes
After reading this article, professionals will be able to:
- Identify the types of noise most common in modern classrooms.
- Recommend specific hearing solutions for individuals with limited useable hearing unilaterally (LUHU).
- Describe the benefits of CROS systems for students with LUHU.
 Erin Picou
Erin Picou 1. The past few months I’ve seen several children with SSD and I’m not sure what exactly are the best treatment options? Is that something we can discuss?
Most certainly. There have been new research insights in the last couple of years on this topic. But before we get into the research, I would like to talk about the term single-sided deafness or “SSD.” This term has often been used to describe a person’s hearing loss when they have normal hearing in one ear and profound hearing loss, very poor word recognition performance, and/or marked intolerance to sounds in the other ear (Valente et al., 2006). However, the term SSD isn’t very descriptive audiologically because it describes a number of different configurations (Cire, 2012). In recognition of this, Bagatto and colleagues suggest using the term “profound unilateral hearing loss” (2019). That term, however, doesn’t capture all variations of SSD, nor does it provide insight into the patient’s listening needs. As a result, we have recently started referring to this type of hearing loss as “limited useable hearing unilaterally” or LUHU. Ultimately, what’s important is that we all understand the patient’s listening needs. Whether we call this configuration SSD, LUHU, or even profound unilateral hearing loss, it seems clear that this type of unilateral hearing loss is generally not aidable. It usually is difficult to provide adequate gain to improve effective audibility for speech sounds, especially while maintaining comfort.
2. You’re right. The patients I’m referring to usually have a severe-to-profound loss and very poor word recognition, and therefore, are poor candidates for traditional amplification. Would you agree that an FM system is the best choice?
Sometimes. FM systems, or the more generic term, remote microphone (RM) systems are certainly a great choice for school-aged children in classrooms who will accept the systems. Indeed, most current guidelines and recommendations suggest RM systems offer the most consistent benefits relative to other non-surgical options (American Academy of Audiology, 2013; Lieu, 2015; McKay et al., 2008). Thus, it is not surprising that RM systems are a very popular treatment option for children with LUHU.
3. What other non-surgical options are there?
The easiest intervention is to do nothing and simply monitor a child’s listening needs and academic performance. Many children with LUHU can be academically successful and do not require intervention. However, there are clear downsides to such a failure-based approach. Approximately 30% of children with unilateral hearing loss will struggle academically (Bess & Tharpe, 1984; Lieu, 2004), and waiting for that to happen puts the children who do struggle at a disadvantage if we only intervene once they start to struggle. One way to prevent academic difficulties would be to make listening in classrooms easier. Especially in noisy situations when speech is near the ear with hearing loss, understanding speech for students with LUHU is likely to be difficult (Bess et al., 1986; Lieu et al., 2013) and effortful (Oosthuizen et al., 2021b). As a result, I recommend exploring options for improving speech recognition and listening effort. Non-surgical options to address LUHU include RM systems, as I have already mentioned, in addition to preferential seating and contralateral routing of signals (CROS) systems.
4. Preferential seating simply means moving the student closer to the teacher, correct?
Exactly. The generic recommendation of moving the student close to the teacher is a great recommendation when trying to maximize the audibility of the teacher’s voice. However, for students with LUHU, we should think about preferential seating more broadly and take into consideration all of the potential talkers of interest in the classroom. Figure 1 illustrates the expected audibility or speech intelligibility for all of the talkers in a hypothetical classroom for a student with LUHU in the right ear. In this example, the student can hear the peers in the front and on the left pretty well (as indicated by green desks), and can hear the teacher fairly well (light orange desk). Conversely, peers closer to the ear with LUHU will be very difficult to understand (as indicated by red desks). As you can see, what is “preferential” for this student will depend on who is talking and who the student is interested in hearing. By moving the student to the front of the classroom, the teacher’s desk would become green, but more of the peer desks would become red. In order to maximize intelligibility for all of the talkers in the classroom, we would need to combine preferential seating with something else, like a RM or CROS system.
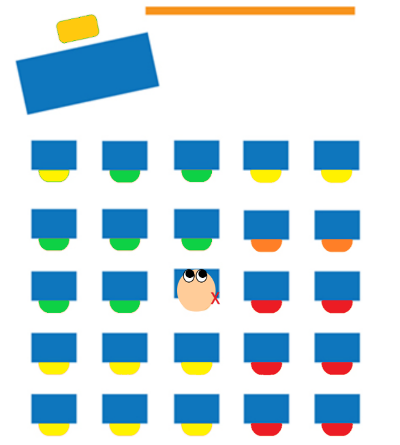
Figure 1. Schematic diagram of classroom. A student with right LUHU is shown. Expected speech recognition for people sitting at each desk are indicated by color coding: Green=Good, Yellow=Moderate, Orange=Fair and Red=Poor.
5. CROS systems? I recall being told that they didn't work very well?
I don’t know how long it’s been since you’ve worked with CROS systems, but before I respond to your comment, let me talk just a little bit about the CROS hearing aids of today—things have changed considerably since the days when we ran a wire through the frame of bulky eyeglasses. The basic acoustic goal of course is the same. We have a transmitter microphone on the ear with LUHU, which (wirelessly) sends the signal to the other side of the head, where it is channeled into the ear with better hearing. If the patient has normal hearing in this ear, which usually is the case, the amount of gain applied usually is minimal (just enough to eliminate the head-shadow effect). Most CROS hearing aids today have the same form factors and features that you will find with traditional products from the same manufacturer (e.g., directional technology, noise reduction, connectivity, rechargeable, etc.).
Now, back to your question. Yes, you’re correct, the prevailing wisdom encourages us to be very careful about fitting CROS systems on children, especially those who might not orient themselves to optimize their listening situation (American Academy of Audiology, 2013; Lieu, 2015; McKay et al., 2008). Those recommendations were based on a couple of laboratory studies, which demonstrated CROS benefits when speech was near the ear with LUHU (a “monaural indirect” listening situation), but significant CROS detriments when the speech was near the ear with normal hearing (a “monaural direct” listening situation; Kenworthy et al., 1990; Updike, 1994). This makes sense if we look back at Figure 1. A CROS would help turn those red desks to the student’s right side from red to yellow or even green. However, the desks on the left side are already green; there’s not much for the CROS system to do. Additionally, if there is an air conditioner over by the red desks (or the children in the red desks are making a ruckus), a CROS system would route those unwanted sounds to the ear with normal hearing, making listening more challenging. We might expect to see those green desks turn to yellow or orange, depending on what sort of noise was coming from the right side.
6. So an RM system would work better?
With an RM system, the remote microphone would significantly improve the signal-to-noise ratio (SNR) for the teacher’s voice, no matter where the teacher was located. In Figure 1, the teacher’s desk would change from orange to green. Importantly, the benefits of RM systems are not location dependent; no matter where in the classroom the teacher was as long as they had the remote microphone, the teacher’s voice would always be easy to hear. Indeed, with a remote microphone near the talker of interest, RM systems have been shown to improve speech recognition performance (Kenworthy et al., 1990; Updike, 1994) and to reduce the mental effort associated with listening (Oosthuizen et al., 2021a) for children with LUHU.
7. But what about the voices of other students in the classroom?
Although we would expect that other students would sometimes generate unwanted “noise” (e.g., talking out of turn), there are many occasions where the students themselves become talkers of interest (e.g., class discussions or “popcorn” reading exercises). In modern classrooms, we see many of these interactive, multiple talker situations; they often outnumber traditional “teacher in front” listening scenarios (Jones, 2016; Ricketts et al., 2010). Therefore, I think it is critically important for us to evaluate how these systems work in multi-talker listening situations, not only traditional single-talker scenarios.
8. What sort of listening scenarios were included in those early studies with CROS and RM systems you mentioned?
The two most relevant laboratory studies both focused on single talker scenarios where the remote microphone was always near the speech signal (Kenworthy et al., 1990; Updike, 1994). They also used noise that was primarily directional (it originated mostly from the side or from the back). The directional noises are informative, but they, too, are only one type of noise students experience in classrooms. More commonly, classrooms are full of noise that comes from many different directions and surrounds students (Ricketts et al., 2010). Thus, modern classrooms have diverse listening situations, the most common of which were not evaluated in early investigations of CROS and RM systems. Moreover, technology has changed significantly since the time that many of these studies were conducted.
9. Are there more recent studies examining different types of listening situations that can expand our understanding of the benefits and limitations of CROS and RM systems?
We do have some more recent data. A couple of years ago, I was lucky to team up with Dr. Tharpe in my department at Vanderbilt University Medical Center (VUMC) and Dr. Dawna Lewis at Boys Town National Research Hospital. Together, with the help of some stellar clinicians (Drs. Gina Angley and Hilary Davis at VUMC), we designed a series of laboratory studies examining the potential for CROS and RM systems in dynamic listening situations with multiple talkers and noise that surrounded a participant (Picou et al., 2020a; Picou et al., 2020c). We tested school-aged children in a couple of different scenarios, including with the loudspeaker array displayed in Figure 2. In the figure, you’ll see the color-coded speech loudspeakers, which presented speech one sentence at a time, but interleaved so the participant did not know where the next sentence was coming from. Students completed testing without an assistive technology (unaided), with a CROS system, and with a RM system. To be consistent with a classroom scenario with only a single microphone, we left the remote microphone near the front loudspeaker.
10. What did you find?
As you can see in Figure 2, we found that, regardless of where the speech was originating, performance with the CROS system was the best, hovering near the ceiling for all loudspeaker locations. As expected, students had difficulty when the loudspeakers were directed towards the ear with LUHU without an intervention system. Importantly, the performance was actually the worst with the RM system for those side and side-back loudspeakers. This is because the remote microphone stayed near the talker of interest and there was no mechanism for routing the speech to the ear with normal hearing with only the RM system. Importantly, we do not see a disadvantage of CROS use for any of the loudspeaker locations. This is inconsistent with the traditional wisdom that CROS can impair speech recognition if listening is already easy and the CROS routes noise to the ear with normal hearing. For the front and front-side loudspeaker conditions, we might expect CROS to impair speech recognition if the concern generalized from directional (or targeted) noises to noises that surround a listener. But we don’t see that here. CROS only provided benefits.
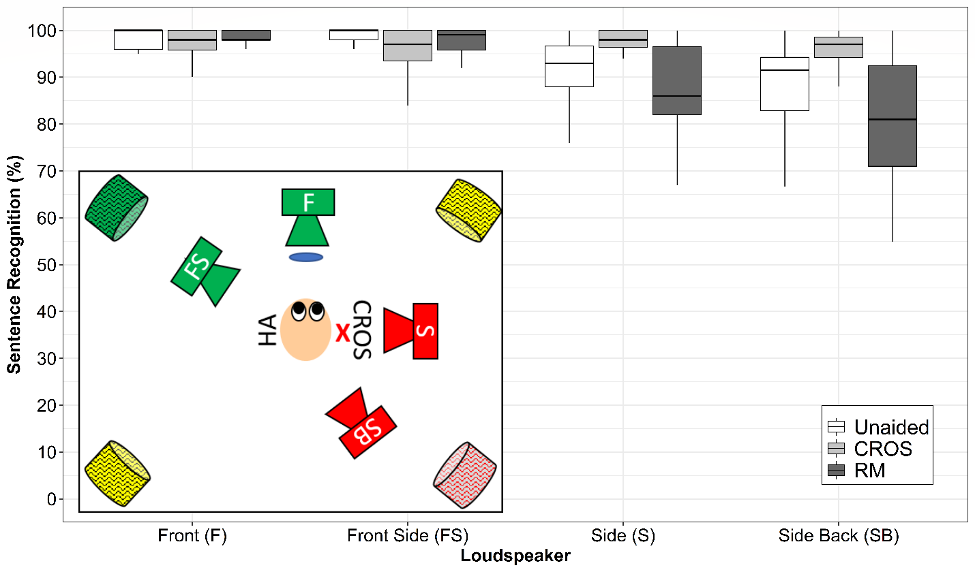
Figure 2. Loudspeaker setup (inset) and results from Picou et al. 2020c. Colors indicate expected audibility, consistent with Figure 1. Blue circle indicates position of the remote microphone. Red X indicates LUHU. Speech loudspeakers are indicated with letters for their location and noise loudspeakers are indicated by hash marks. Figure is not to scale.
11. This makes sense, but these conditions seem like they were designed to highlight the strengths of the CROS system?
We also looked at alternative scenarios where CROS would be expected to be less helpful. We evaluated a mirrored loudspeaker set up, pictured in the inset of Figure 3, where we would expect the CROS system to reduce sentence recognition. We still don’t see evidence that CROS impaired speech recognition performance. Also, the RM system did not provide benefits for the loudspeaker location where the students were most likely to have difficulty (front-side in Figure 3). Based on this pattern of results, I believe CROS systems can help students with LUHU in many modern classroom scenarios. I also believe the earlier laboratory studies over-estimated the negative consequences of CROS use in monaural direct listening situations.
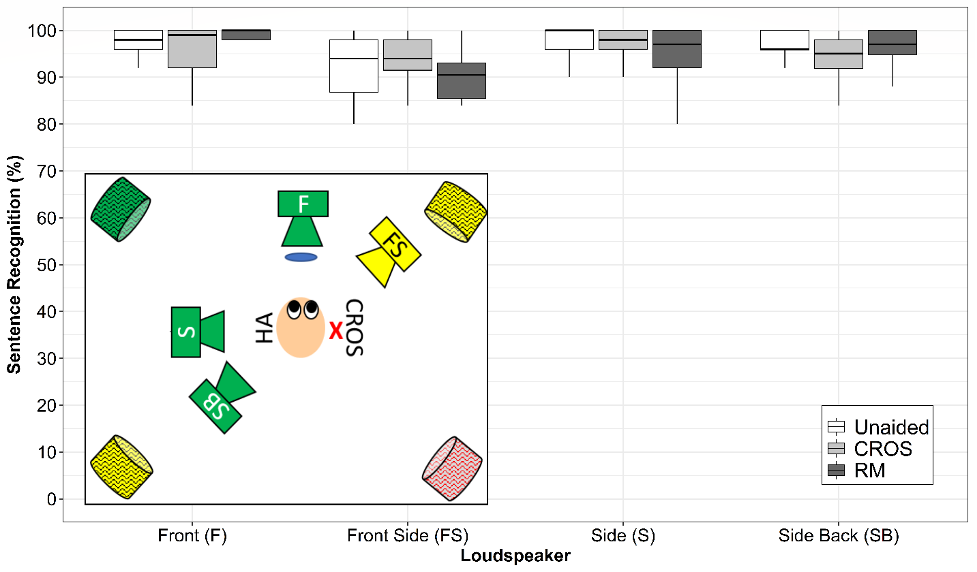
Figure 3. Loudspeaker setup (inset) and results from Picou et al. 2020c. Colors indicate expected audibility, consistent with Figure 1. Blue circle indicates position of the remote microphone. Red X indicates LUHU. Speech loudspeakers are indicated with letters for their location and noise loudspeakers are indicated by hash marks. Figure is not to scale.
12. Is there data to support the use of CROS systems outside the laboratory?
Yes. We recently completed a narrative review of non-surgical interventions for students with LUHU and we identified several questionnaire-based studies that demonstrate the benefits of CROS use (Picou et al., 2020b). A couple of these studies were published more than 40 years ago (Miller, 1967; Shapiro, 1977), and CROS technology has advanced considerably since these studies were published. To see if modern systems help in real classrooms, we asked the established CROS users in our studies to rate their perceived CROS benefits using a questionnaire developed for our project. The participants nearly unanimously agreed that their CROS hearing aids helped them understand talkers in the front and from behind, although most did not report the CROS system helped in situations where localizing was important. Their subjective reports are consistent with the laboratory data and also consistent with our expectations about CROS. Because sounds are being re-routed to a single ear, the systems do not provide a listener with binaural hearing.
13 How would I help my patient with LUHU improve localization?
Currently, the only way to give a patient with LUHU bilateral hearing would be through cochlear implantation. Relatively recently, cochlear implantation has become a possibility for people with unilateral hearing loss, but of course there are a myriad of considerations for determining implant candidacy, including duration of hearing loss (Bagatto et al., 2019). For people who are candidates, cochlear implantation has been able to improve spatial hearing (Bernstein et al., 2017) and speech recognition in noise (Hassepass et al., 2013).
14. Are there other surgical options?
The other surgical option, bone conduction hearing aids, can be implanted or they can be attached with a soft-band headband or more recently adhesive (Dahm et al., 2018). The rationale behind bone conduction hearing aids is pretty similar to CROS systems and, therefore, most of the learnings we have about CROS systems benefits should also apply to bone conduction devices. Indeed, outcomes with CROS and bone conduction devices can be pretty similar for people with LUHU (e.g., Snapp et al., 2017). There are, of course, differences between CROS systems and bone conduction devices. For example, the frequency response of a CROS system is broader and not limited by skull vibration (Choi et al., 2019). Conversely, bone conduction devices leave the ear canals unoccluded, and thus sound can enter the ear canal of the ear with normal hearing without amplification or attenuation.
15. You raise an interesting point about the attenuation of sounds. What causes signal attenuation?
The coupling to the hearing aid with the CROS receiver can attenuate the incoming signal. Even if the receiver is an “open fit” instrument, the size of the patient’s ear canal and the size of the ear tip will interact and could cause some insertion loss, especially in the high frequencies. Especially because a patient with LUHU only has useable hearing in one ear, it is critically important to limit the insertion loss by using coupling that is as open as possible.
16. Are there other ways to overcome the insertion loss you mention?
Yes. You could program the CROS receiver instrument to have 0 dB insertion gain to overcome this insertion loss. In this case, you would have actually fit a BiCROS system, or a “bilateral contralateral routing of signals” system. Most of the CROS systems I have worked with lately have actually been a BiCROS (microphone also on ear with better hearing), we simply did not use the hearing aid except to compensate for insertion loss. This of course assumes that you are using probe-microphone verification when fitting CROS instruments.
17. So should we be fitting BiCROS on everyone?
I have not seen any evidence in support or against this idea. It makes sense to me that we want to limit the potential harms caused by fitting a CROS system, including insertion loss. So, fitting a BiCROS and compensating for insertion loss seems like a good idea. Similarly, if the patient has hearing loss in their better hearing ear, a BiCROS system would be able to provide benefits of a CROS system while also aiding the better hearing ear (e.g., Petrausch et al., 2016). Routinely fitting BiCROS systems also would allow you to use the same system if the hearing person’s better hearing ear hearing declines.
18. This information makes CROS systems look more favorable than I would have anticipated. Should we abandon the RM systems for patients?
Definitely not. RM systems are still our best method of improving the SNR and overcoming distance effects. They are limited by the number of microphones available. In the classroom, with only a single microphone, CROS systems can offer benefits in multi-talker situations for people with LUHU, benefits that might elude single-microphone RM systems. Figure 4 displays schematic diagram of a classroom with a student in the center using either RM system (left panel) or CROS system (right panel), based on the updated laboratory studies I mentioned. As you can see, neither solution is expected to provide excellent speech intelligibility for all talkers in the classroom. The RM system is most beneficial for the teacher’s voice and the CROS system is most beneficial for the peers’ voices.
Note that the scenarios we have been discussing also assume that a student could only use an RM or a CROS system, not both simultaneously. As the technology advances, I hope we will see the possible combination of RM and CROS systems, which would offer the benefits of both systems to patients with LUHU. It will probably require a combination system, and/or multiple remote microphones, to turn all of the desks in Figure 4 to green.
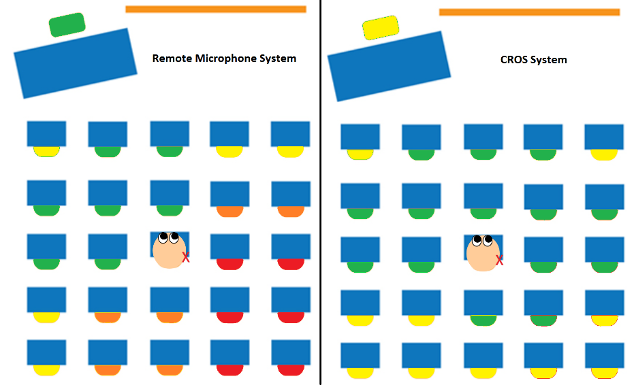
Figure 4. Schematic classroom diagrams with hypothetical RM system (left panel) and CROS system (right panel). Color coding and symbols are the same as in Figure 1.
19. Back to my original question, my patients with LUHU use personal RM systems in the classroom. Should I change their management plan?
I think you could consider trying a CROS system. Modern CROS systems have proven advantages in dynamic classroom listening scenarios and the disadvantages of CROS systems are not be as significant we previously thought. I would also investigate their specific classroom arrangement(s) and consider recommending a different preferential seat. Your recommendation will depend also on the intervention they are using, and the location of the most common noises. In our review, we explore some of the factors that could affect seat recommendations, which I encourage you to check out if you are considering preferential seat recommendations (Picou et al., 2020b).
20. Is there a way to predict who will benefit from a CROS system?
This is an excellent question because some patients with LUHU who try CROS system (and RM systems for that matter) prefer to use nothing instead of these potentially cumbersome technologies. Recent evidence in adults suggest that, after trialing a RM system, a bone conduction device, and a CROS system, most participants (53%) chose to keep the CROS system. Only 2 of 15 participants chose to use the RM system and 3 chose to continue with no intervention (Fogels et al., 2020). It would be fabulous to have the ability to predict, based on some clinical measure or questionnaire, whether or not a student will report benefit from a CROS system before we invested resources into fitting them. We are working now on a project investigating the potential for a questionnaire we developed to predict CROS system acceptance. The preliminary data look promising and maybe we can discuss our findings sometime soon.
References
American Academy of Audiology. (2013). American Academy of Audiology clinical practice guidelines: Pediatric amplification. Reston, VA: American Academy of Audiology.
Bagatto, M., DesGeorges, J., King, A., Kitterick, P., Laurnagaray, D., Lewis, D., et al. (2019). Consensus practice parameter: Audiological assessment and management of unilateral hearing loss in children. International Journal of Audiology, 1-11. https://doi.org/10.1080/14992027.2019.1654620
Bernstein, J. G., Schuchman, G. I., & Rivera, A. L. (2017). Head shadow and binaural squelch for unilaterally deaf cochlear implantees. Otology & Neurotology, 38, e195-e202.
Bess, F. H., & Tharpe, A. M. (1984). Unilateral hearing impairment in children. Pediatrics, 74, 206-216.
Bess, F. H., Tharpe, A. M., & Gibler, A. M. (1986). Auditory performance of children with unilateral sensorineural hearing loss. Ear and Hearing, 7, 20-26. https://doi.org/10.1097/00003446-198602000-00005
Choi, J. E., Ma, S. M., Park, H., Cho, Y.-S., Hong, S. H., & Moon, I. J. (2019). A comparison between wireless cros/bicros and soft-band baha for patients with unilateral hearing loss. PLoS One, 14, e0212503.
Cire, G. (2012). Understanding single sided deafness: Evaluation and treatment for professionals. AudiologyOnline.
Dahm, V., Baumgartner, W.-D., Liepins, R., Arnoldner, C., & Riss, D. (2018). First results with a new, pressure-free, adhesive bone conduction hearing aid. Otology & Neurotology, 39, 748-754.
Fogels, J., Jönsson, R., Sadeghi, A., Flynn, M., & Flynn, T. (2020). Single-sided deafness—outcomes of three interventions for profound unilateral sensorineural hearing loss: A randomized clinical trial. Otology & Neurotology, 41, 736-744.
Hassepass, F., Aschendorff, A., Wesarg, T., Kröger, S., Laszig, R., Beck, R., et al. (2013). Unilateral deafness in children: Audiologic and subjective assessment of hearing ability after cochlear implantation. Otology & Neurotology: official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology, 34, 53-60.
Jones, C. (2016). Legit innovation for teens. Paper presented at the 7th International Pediatric Audiology Conference, Atlanta, GA.
Kenworthy, O., Klee, T., & Tharpe, A. (1990). Speech recognition ability of children with unilateral sensorineural hearing loss as a function of amplification, speech stimuli and listening condition. Ear and Hearing, 11, 264-270. https://doi.org/10.1097/00003446-199008000-00003
Lieu, J. E. (2015). Management of children with unilateral hearing loss. Otolaryngologic Clinics of North America, 48, 1011-1026. https://doi.org/10.1016/j.otc.2015.07.006
Lieu, J. E., Karzon, R. K., Ead, B., & Tye-Murray, N. (2013). Do audiologic characteristics predict outcomes in children with unilateral hearing loss? Otology & Neurotology, 34, 1703. https://doi.org/10.1097/MAO.0000000000000190
Lieu, J. E. C. (2004). Speech-language and educational consequences of unilateral hearing loss in children. Archives of Otolaryngology–Head & Neck Surgery, 130, 524-530.
McKay, S., Gravel, J. S., & Tharpe, A. M. (2008). Amplification considerations for children with minimal or mild bilateral hearing loss and unilateral hearing loss. Trends in Amplification, 12, 43-54. https://doi.org/10.1177/1084713807313570
Miller, A. L. (1967). Body type hearing aids for unilateral hearing losses. Journal of Speech Hearing Disorders, 32, 268-269. https://doi.org/10.1044/jshd.3203.268
Oosthuizen, I., Picou, E. M., Pottas, L., Myburgh, H. C., & Swanepoel, D. W. (2021a). Listening effort in school-aged children with limited useable hearing unilaterally: Examining the effects of a personal, digital rm system and a cros system. Trends in Hearing, 25, 1-16. https://doi.org/10.1177/2331216520984700
Oosthuizen, I., Picou, E. M., Pottas, L., Myburgh, H. C., & Swanepoel, D. W. (2021b). Listening effort in school-aged children with normal hearing compared to children with limited useable hearing unilaterally. American Journal of Audiology.
Petrausch, S., Manders, A., & Jacobus, K. (2016). A new wireless cros and bicros solution. Canadian Audiologist, 3.
Picou, E. M., Davis, H., Lewis, D., & Tharpe, A. M. (2020a). Contralateral routing of signals systems can improve speech recognition and comprehension in dynamic classrooms. Journal of Speech, Language & Hearing Research, 63, 2468-2482. https://doi.org/10.1044/2020_JSLHR-19-00411
Picou, E. M., Davis, H., & Tharpe, A. M. (2020b). Considerations for choosing microphone technologies for students with limited useable hearing unilaterally. Language, Speech, and Hearing Services in Schools, 51, 74 - 83. https://doi.org/10.1044/2019_LSHSS-OCHL-19-0018
Picou, E. M., Lewis, D., Angley, G., & Tharpe, A. M. (2020c). Rerouting hearing aid systems for overcoming limited useable unilateral hearing in dynamic classrooms. Ear and Hearing, 41, 790-803. https://doi.org/10.1097/AUD.0000000000000800
Ricketts, T. A., Picou, E. M., Galster, J. A., Federman, J., & Sladen, D. P. (2010). Potential for directional hearing aid benefit in classrooms: Field data. In R. C. Seewald & J. Bamford (Eds.), A sound foundation through early amplification (pp. 143-152). Chicago, IL: Phonak, AG.
Shapiro, I. (1977). Children's use of cros hearing aids. Archives of Otolaryngology, 103, 712-716. https://doi.org/10.1001/archotol.1977.00780290048005
Snapp, H. A., Holt, F. D., Liu, X., & Rajguru, S. M. (2017). Comparison of speech in noise and localization benefits in unilateral hearing loss subjects using contralateral routing of signal hearing aids or bone anchored implants. Otology & Neurotology: official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology, 38, 11.
Updike, C. D. (1994). Comparison of fm auditory trainers, cros aids, and personal amplification in unilaterally hearing impaired children. Journal of the American Academy of Audiology, 5, 204-209.
Valente, M., Valente, M., & Mispagel, K. (2006). Fitting options for adult patients with single sided deafness (ssd). AudiologyOnline.
Citation
Picou, E. (2021). 20Q: Amplification considerations for unilateral hearing loss - A case for CROS. AudiologyOnline, Article 27784. Available at www.audiologyonline.com

