 From the Desk of Gus Mueller
From the Desk of Gus Mueller
Noted audiology and hearing science researcher Anna Karczewska-Nabelek died last month at the age of 81. Going back to 1973 until her retirement just a few years ago, Dr. Nabelek was a faculty member at the University of Tennessee in Knoxville. Her many publications spanned four decades. Among her Acoustical Society colleagues, she was particularly known for her seminal work regarding speech recognition in noise and reverberation. However, among clinicians, Dr. Nabelek was mostly known for her body of research that utilized a speech test that did not relate to speech recognition . . . at least not directly.

Gus Mueller
In 1991, Dr. Nabelek was the senior author of a paper entitled, “Toleration of background noises: Relationship with patterns of hearing aid use by elderly persons.” The article brought forth the concept that while we normally think of benefit and satisfaction with hearing aids as being related to speech understanding, the patient’s ability to tolerate background noise also may play an important role. Other studies relating an individual’s “tolerated noise” to hearing aid use were conducted at the University of Tennessee in the 1990s. They revealed that these noise tolerance levels were mostly unrelated to aided speech recognition in noise, and indeed, may serve as a unique predictor of hearing aid success. Somewhere along the way, this noise tolerance test became known as the Acceptable Noise Level, or simply the ANL.
The ANL found its way out of Knoxville in the 2000s, and quickly became the focus of research around the world. Since 2004, there have been 44 peer-reviewed papers on the ANL, and at least another 10 or more data-based articles in non-refereed journals. What other audiologic behavioral test has been subjected to this amount of research in a ten-year span? What is it about the ANL that makes it so interesting? Well, we’re about to find out!
Our guest at 20Q this month is Patrick Plyler, PhD, who comes to us directly from ANL-Land. He is Professor in the Department Audiology and Speech Pathology at the University of Tennessee, and Director of the UT Hearing Instrument Research Laboratory. Dr. Plyler worked with Dr. Nabelek for many years, and has been involved with numerous ANL research projects over the past two decades.

ANL research team circa 2005. Dr. Nabelek (center) is surrounded
by audiologists Melinda Freyaldehoven (left), this month’s 20Q author
Patrick Plyler (top) and Joanna Tampas (right).
In addition to his ANL research, Dr. Plyler has published extensively in the areas of hearing aid technology and speech perception. He’s actively involved in the AuD and PhD programs at UT, and has been acknowledged on several occasions for his teaching excellence. He holds numerous awards for his published articles and his journal editing services.
With over 50 articles on the topic, there certainly is a lot to say about the ANL. It quickly became obvious that everything that needed to said couldn’t be brought forward in 20 questions. This month’s 20Q, therefore, is the first of two on the topic. In this initial installment, Patrick nicely explains the test rationale, and provides all the clinical tips needed for conducting and interpreting the test the right way. This will be enough to get you started—see you next month for a deeper dive into the ANL background research.
Gus Mueller, PhD
Contributing Editor
June, 2015
To browse the complete collection of 20Q with Gus Mueller CEU articles, please visit www.audiologyonline.com/20Q
20Q: Acceptable Noise Level Test - The Basics and Beyond
Learning Objectives
- Describe the background and purpose of the Acceptable Noise Level (ANL) Test.
- Explain how to conduct the ANL test with patients.
- Discuss interpretation of ANL scores and how they may impact clinical management.

Patrick Plyler
1. I certainly have heard of the ANL test, but to be honest, I don’t know much about it. Can we start at the beginning?
Sure. The Acceptable Noise Level (ANL) was developed at the University of Tennessee by my colleagues Anna Nabelek and Sam Burchfield back in the early 1990s. They were questioning if there was some measure that we could do clinically, that might help predict success with hearing aids. The development process started with some general observations.
2. Such as?
There actually were three observations that led to the ANL development.
The first observation was that hearing aid users commonly complained about background noise (Kochkin, 2002a; Kochkin, 2002b). Therefore, it seemed reasonable that background noise, in some way, probably was related to hearing aid use.
Secondly, previous research had not documented a relationship between speech-in-noise performance and hearing aid success or rejection (Bentler, Niebuhr, Getta, & Anderson, 1993; Humes, Halling, & Coughlin, 1996). It seemed strange that complaints about background noise and speech perception in background noise were unrelated.
The third observation involved statements made by hearing aid outcome investigators concerning the need for more objective measures that correctly predicted hearing aid use (Garstecki & Erler, 2003; Nemes, 2003).
3. Before you go on, did I hear you say that speech-in-noise performance may not be related to hearing aid success?
I did say that. Of course, we all know that improving speech perception is an important goal of any hearing aid fitting. One would therefore assume that improved speech perception with hearing aids would be associated with better utilization of hearing aids. Although research routinely shows that hearing aids improve speech perception, neither speech perception scores in quiet or in background noise seem to impact hearing aid use, or at least not to the extent that we would expect (Bentler et al., 1993; Humes et al., 1996). Consequently, Dr. Nabelek questioned if an individual's willingness to listen in background noise may be more indicative of hearing aid use than actual speech understanding (Nabelek, Tucker & Letowski, 1991). In other words, hearing aid use appeared to be related to the acceptance of background noise instead of speech understanding in quiet or in noise. So, any improvement in speech perception obtained when using hearing aids becomes irrelevant if the listener is unwilling to wear hearing aids in a particular listening environment.
4. I see. Does research suggest that an individual’s ANL may be related to hearing aid use?
Yes. We can go into in more detail later if you like, but the initial ANL research demonstrated that background noise acceptance is related to hearing aid use. Individuals who accept background noise (small ANL) have a better chance of being successful hearing aid users, and the opposite if also true. Individuals who are willing to accept less background noise (large ANL) will probably be unsuccessful hearing aid users (Nabelek et al., 1991; Lytle,1994; Nabelek, Freyaldenhoven, Tampas, & Burchfield, 2006; Freyhaldenhoven, Plyler, Thelin, & Muenchen, 2006). The probability of being a successful hearing aid user decreases as the unaided ANL value increases (gets worse).
5. Sounds like good information to have. What exactly is the ANL test and how do I do it?
The ANL test determines the highest background noise level a listener deems acceptable while listening to speech at their most comfortable level (MCL). To begin, the listener adjusts recorded running speech to their MCL through a modified method of adjustments. Next, a multi-talker babble is added to the speech. The listener adjusts the babble to the highest level that enables them to follow the speech passage without becoming tense or tired, in other words, to the highest level that they are willing to “put up with”. This determines the background noise level or BNL.
6. Sounds simple enough, but how is the ANL determined?
The ANL is simply the difference between MCL for speech and the BNL. In other words, ANL=MCL-BNL (all in dB). For example, if the patient's MCL is 75 and the BNL is 70, then the patient's ANL would be 5 dB. It is best to conduct the test at least 2 times for accuracy and reliability.
7. But that sounds like a signal-to-noise ratio (SNR), not a “level?”
You’re right, we do calculate an SNR. Early on, the terms “tolerated speech-to-noise ratio” were used to describe the measurement. Later, it was decided to refer to it as a level, and that helped differentiate the procedure from other SNR tests of speech recognition.
8. Isn’t it somewhat difficult to find someone’s MCL?
Well, it’s easy to do the test, but also easy to record the wrong value if you’re not careful. The problem is that the MCL isn’t really a precise dB level, but rather a dB range, which often is 6-10 dB or so for people with cochlear hearing loss. For this reason, the testing must be conducted carefully, and audiologists must do their best to find the center of that range. That’s why I also mentioned the importance of repeating the testing.
9. I’d guess the instructions also are important?
Absolutely. If you don’t use the correct instructions, you might as well not do the test, as the findings probably won’t be valid or reliable. In the research lab, we use handheld buttons in test booth, so that the patients can control the loudness themselves, and our instructions relate to this procedure (Nabelek, Tampas, & Burchfield, 2004). I realize it’s unlikely that you will this apparatus in your clinic, so I’ve included adapted instructions that involve the patient simply making hand gestures to the clinician to have the signal turned either louder or softer. Thumb up for louder, thumb down for softer, and good strong head nod or flat palm for “just right” usually works pretty well (Gordon-Hickey & Moore, 2007). We suggest starting at around 30 dB HL and initially using 5-dB steps to find the general upper and lower limits. After that, be sure to conduct a final bracketing approach using 2 dB steps.
Instructions for Establishing Most Comfortable Listening Level. You will listen to a story through a loudspeaker. After a few moments, select the loudness of the story that is most comfortable for you, as if listening to the radio. The thumbs-up and thumbs-down gestures will allow you to make adjustments. First, turn the loudness up until it is too loud and then down until it is too soft. Next, select the loudness level that is most comfortable to you.
Instructions for Establishing Background Noise Level. You will listen to the same story with background noise of music or several people talking at the same time. After you have listened to this for a few moments, select the level of background noise that is the MOST you would be willing to accept or “put up with” without becoming tense and tired while following the story. First, I'll turn the noise up until you let me know that it is too loud (thumbs down) and then I'll turn it down until the story becomes very clear (thumbs up). Next, I'll adjust the noise (up and down) to the MAXIMUM noise level you would be willing to “put up with” for a long time while following the story.
These instructions were adapted from Nabelek, Tampas, et al (2004).
10. Those instructions look pretty straightforward. Anything special about the instructions I should remember?
What tends to cause the most problems is the patient’s understanding of how to set the levels for both the speech in quiet and the background noise. It is important the patient experiences a range of levels before settling in on their final MCL and BNL values. Often times a patient just increases the speech or the noise a few dB and stops, without experiencing levels that are unacceptable to them, both for too loud and too soft. Before giving the instructions, I often give the example of the three little bears in that we are trying to identify the levels that are “too hot, too cold, and just right.” That seems to helps most patients. For patients still having trouble, I suggest using a three-staged approach for both the MCL and BNL measures. Provide instructions for increasing the level that is too loud and complete that task. Next, provide instructions for decreasing the level that is too soft and complete that task. Lastly, provide instructions for finding the acceptable level and complete the task.
11. Do I need to conduct ear-specific measures using earphones, or is the test conducted in the soundfield?
If you’re somewhat limited for time, simply doing bilateral measures in the soundfield probably will be okay. Hearing loss has little impact on the ANL, so even if ear asymmetry is present, it shouldn’t be a big factor. For most patients, ANL values do not improve when tested bilaterally (versus unilaterally); however, intra-aural differences do exist for a small percentage of patients, even when hearing loss is the same in both ears. In the case of a unilateral hearing aid fitting, it may be wise to measure ANLs monaurally using earphones to determine if an intra-aural difference exists. If so, consider fitting the ear with the lower ANL (Freyhaldenhoven, Plyler, Thelin, & Burchfield, 2006.)
12. How long will ANL testing take?
The time investment is minimal, especially when you consider that you may be learning information about the patient not available from the findings of any other test. If it’s a typical patient, and you conduct the ANL in the soundfield and repeat the measure to assure reliability, you’re probably looking at 5 minutes. If you conduct ear-specific testing, then add a few minutes more.
13. This seems like a pretty unique measure for the patient. Can I be confident that the findings are reliable?
A reasonable question and this certainly has been studied. Like any of the behavioral tests that we do, there will be a few patients who just won’t understand the task, but this is rare. In general, research has shown that test-retest reliability is quite good.
Mueller, Weber and Hornsby (2006) examined the reliability of just the BNL, which these authors believed had the greatest variability. They found that when repeating the BNL three different times for 22 participants, in 15% of the comparisons the BNL did not change at all for a given individual. In 61% of the comparisons, it only changed by 2 dB. The largest intra-subject difference was 6 dB, observed for 11% of the comparisons.
Interestingly, a recent study evaluated the intertester reliability of the ANL by completing the test using 3 different examiners. Mean MCL values averaged across participants for each examiner were 48.7, 49.2, and 49.6 dB HL. Similarly, mean ANL values were 3.7, 4.5, and 4.4 dB. These researchers concluded that the MCL, BNL, and ANL can be reliably measured across testers, laboratories, and clinics, provided the ANL instruction set is accurately followed (Gordon-Hickey et al., 2012).
14. Once I’ve completed the testing, how do I interpret the ANL value I’ve obtained?
Well for starters, simply remember that the higher the ANL value, the worse it is for the listener. Listeners with high ANL values accept less noise while listeners with low ANL values accept more noise. In the 25 years of research at our laboratory, we have found ANL values that range from -2 to 38 dB in listeners with normal hearing and from -2 to 29 dB in listeners with impaired hearing. The most frequently observed ANL value is around 10 dB for both groups of listeners (Nabelek et al., 2004).
15. You say that some people with hearing loss have ANL values as small as -2 dB? And as large as 29 dB?
True, but keep in mind these are the extreme cases and the datasets for these initial studies were very large. In fact, 221 listeners with normal hearing and 315 listeners with impaired hearing were included in the original research. Most ANL studies have much smaller sample sizes and many do not follow the ANL instruction set accurately, both of which may explain why the range of ANL values and the mean ANL value varies from study to study. Nonetheless, several studies have tried to explain the large between subject variability on the ANL test.
16. What do you think would be a typical ANL range that I would find with my everyday patients?
There always will be some extremes, but Table 1 shows ANL results that have been reported in some of the research studies from my laboratory where the participants were of a typical clinical caseload.
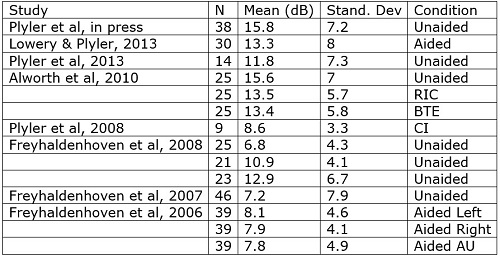
Table 1. ANL results from Dr. Plyer's laboratory utilizing participants from a typical clinical caseload.
17. I understand that small ANLs are good, but at what point should I start to become concerned?
Dr. Nabelek developed some general categories that might be helpful (Nabelek et al., 2006):
ANL Score 7 dB or less: These individuals have a great prognosis for regular use and acceptance of hearing aids; may not need as much follow-up counseling and guidance as the average patient.
ANL Score 8-12 dB: These are your more common patients and have a good (8) or bad (12) prognosis for regular use and acceptance of hearing aids. These patients may need more follow-up counseling and are excellent candidates for noise reduction technologies.
ANL Score 13 dB or more: These patients are “at risk” for reduced utilization of hearing aids and may need additional post-fitting counseling, guidance, and require noise reduction technologies.
18. You mention post-fitting follow-up. Should I do post-fitting ANLs? Do ANLs tend to become smaller as people use their hearing aids more?
Early ANL research suggested ANL values do not change when tested with and without hearing aids over a 3 month time period (Nabelek et al., 2004). This would suggest that hearing aid users do not acclimate to background noise over time, so conducting post fitting testing may not be necessary. That being said, the original ANL work was conducted with hearing aids without digital noise reduction and many without directional microphones. With more modern hearing aids, ANL values could be affected by such features (Lowrey & Plyler, 2013), and if so, post-fitting ANL values could assist with setting the strength of these features. In addition, I believe patients with higher ANL values could possibly see improvements if hearing aids are used over longer time periods than three months, since they have significant room for improvement. I wouldn’t expect to see much change for patients that already accept a lot of noise and have low ANL values.
19. This has been great, and I’m ready to get started. Where do I obtain the test?
Currently, you can obtain the test and an abbreviated set of instructions via Frye Electronics. If you cannot obtain the standard materials and instructions, you may be able to reliably and accurately measure ANL values using various types of running speech samples and various types of background noises (Plyler et al., 2011), assuming speech and noise signals are correctly calibrated and the same ANL instructions are used. Keep in mind the values may not be exactly the same if using different materials, but you could roughly determine a low ANL from a high ANL. We recommend using the standard test materials and instructions if at all possible.
20. I’ll place an order for the CD today. And now I’m ready to hear about all the related research you mentioned.
There is a lot of it, the results of which I think you’ll find both useful and intriguing. How about we do another 20 Questions next month?
References
Alworth, L., Plyler, P., Bertges, M. & Johnstone, P. (2010). The effects of receiver placement on probe microphone, performance and subjective measures with open canal hearing instruments. Journal of the American Academy of Audiology, 21, 249-266.
Bentler, R., Niebuhr, J., Getta, C., & Anderson, C. (1993). Longitudinal study of hearing aid effectiveness. II: Subjective measures. Journal of Speech and Hearing Research, 36, 820-831.
Freyhaldenhoven, M., Plyler, P., Thelin, J., & Burchfield, S. (2006). Acceptance of noise for monaural and binaural hearing aid fittings. Journal of the American Academy of Audiology, 17, 659–666.
Freyhaldenhoven, M., Plyler, P., Thelin, J., & Hedrick, M.S. (2007). The effects of speech presentation level on acceptance of noise in listeners with normal and impaired hearing. Journal of Speech-Language Hearing Research, 50, 878-885.
Freyhaldenhoven, M., Plyler, P., Thelin, J., & Muenchen, B. (2008). Acceptable noise level growth patterns in hearing aid users. Journal of Speech Language and Hearing Research, 51,126-135.
Garstecki, D., & Erler S. (2003). Focused treatment plans for older adults with impaired hearing. ASHA Leader, 8(14),4-5.
Gordon-Hickey, S., Adams, E., Moore, R., Gaal, A., Berry, K., & Brock, S. (2012). Intertester reliability of the acceptable noise level. Journal of the American Academy of Audiology, 23(7), 534–541.
Humes, L., Halling, D., & Coughlin, M. (1996). Reliability and stability of various hearing aid outcome measures in a group of elderly hearing aid wearers. Journal of Speech Language and Hearing Research, 39,923-935.
Kochkin, S. (2002a). 10-year customer satisfaction trends in the US hearing instrument market. Hearing Review, 9(10), 14-46.
Kochkin, S. (2002b). Consumers rate improvements sought in hearing instruments. Hearing Review, 9(11),18-22.
Lowery, K., & Plyler, P. (2013). The effects of noise reduction technologies on the acceptance of background noise. Journal of the American Academy of Audiology, 24(8), 649-659.
Lytle, S. (1994). A comparison of amplification efficacy and toleration of background noise in hearing impaired elderly persons. Unpublished master’s thesis, University of Tennessee, Knoxville.
Mueller, H., Weber, J., & Hornsby, B. (2006) The effects of digital noise reduction on the acceptance of background noise. Trends in Amplification, 10,1–9.
Nabelek, A., Tucker, F., & Letowski, T. (1991). Toleration of background noises: Relationship with patterns of hearing aid use by elderly persons. Journal of Speech and Hearing Research, 34,679-685.
Nabelek, A., Tampas, J., & Burchfield, S. (2004) Comparison of speech perception in background noise with acceptance of background in aided and unaided conditions. Journal of Speech Language and Hearing Research, 47,1001-1011.
Nabelek, A., Freyaldenhoven, M., Tampas, J., & Burchfield, S. (2006). Acceptable noise level as a predictor of hearing aid use. Journal of the American Academy of Audiology, 17(9), 626-639.
Nemes, J. (2003). Despite benefits of outcomes measures, advocates say they’re underused. Hearing Journal, 56(8), 19-25.
Plyler, P., Bahng, J. &, von Hapsburg, D. (2008). Acceptance of background noise in adult cochlear implant users. Journal of Speech Language and Hearing Research, 51,502-515.
Plyler, P., Alworth, L., Rossini, T., & Mapes, K. (2011). Effects of speech signal content and speaker gender on acceptance of noise in listeners with normal hearing. International Journal of Audiology, 50, 243-248.
Plyler, P., Bertges-Reber, M., Kovach, A., Galloway, B., & Humphrey, E. (2013). Comparison of multi-channel wide dynamic range compression and channelfree processing in hearing aids. Journal of the American Academy of Audiology, 24,126-137.
Plyler, P.N., Lang, R., Monroe, A., & Gaudiano, P. (2015). The effects of audio-visual stimulation on the acceptance of background noise in listeners with normal and impaired hearing. Journal of the American Academy of Audiology, 26(5), 451-460.
Cite this Content as:
Plyler, P. (2015, June). 20Q: Acceptable Noise Level Test - The basics and beyond. AudiologyOnline, Article 14403. Retrieved from https://www.audiologyonline.com.

