AudiologyOnline: How does AutoREM work in clinical practice?
Clayton Fisher: AutoREM works by establishing a communication link between the probe microphone system and the hearing aid manufacturer’s fitting software, using a process known as inter-module communication (IMC).
Once the connection is established, the manufacturer’s fitting software initiates a series of aided response measurements using the REM speaker hardware (such as the Inventis Trumpet). These measurements are taken at various input levels and compared to the prescriptive target output across different frequencies.
The software then calculates the error—the difference between the measured output in the patient’s ear canal and the target output and automatically adjusts the hearing aid’s gain settings to align with the prescriptive real-ear targets.
That’s right, AutoREM handles the gain adjustments for you. You can sit back, sip your coffee, and observe the process in action.
AudiologyOnline: Why don’t clinicians use this routinely?
Clayton Fisher: Despite its clear benefits, the adoption of AutoREM among clinicians remains relatively limited.
In my view, the primary reason is that many clinicians, like professionals in any field, are creatures of habit. There’s often a reluctance to adopt new technologies, especially when they involve unfamiliar workflows. The fear of the unknown is likely one of the biggest barriers to broader adoption.
Yet, for many types and configurations of hearing loss, AutoREM offers a significantly faster and more convenient way to ensure hearing aids are fit to prescriptive targets, maximizing both audibility and patient benefit.
That said, AutoREM may not be equally effective across all hearing loss profiles, which can make its application less universal. This variability in effectiveness may contribute to hesitancy in its routine use.
Additionally, compatibility is still a limiting factor: not all hearing aid manufacturers integrate seamlessly with every REM system. For instance, the Inventis Trumpet currently supports AutoREM functionality with the following hearing aid fitting software platforms:
- Starkey Inspire
- Oticon Genie 2
- Beltone SolusMax
- ReSound Smart Fit
- Sonic Innovations EXPRESSfit
- SBO Hearing Philips HearSuite
- Bernafon Oasis NXT
In the next section, I’ll share guidance on when AutoREM is appropriate and when it may not be the best option.
AudiologyOnline: What hearing loss configurations are ideal for the use of AutoREM?
Clayton Fisher: In my clinical experience, AutoREM tends to be most beneficial when the hearing loss is moderate in degree, particularly when there is a low- or mid-frequency component, or when the audiogram presents a relatively flat configuration, including gently rising or sloping patterns.
In particular, I’ve found AutoREM to be highly effective in cases with both downward-sloping and upward-sloping audiograms.
Below are four examples, two of each configuration, where AutoREM played a valuable role in achieving accurate and efficient fittings.
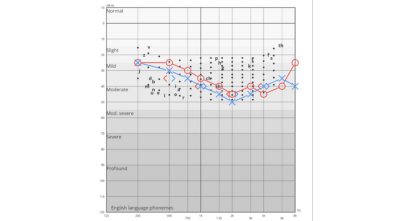
Figure 1. AutoREM performs exceptionally well in cases of mild sloping to moderate sensorineural hearing loss (SNHL).
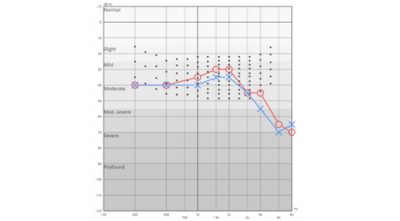
Figure 2. AutoREM is also effective for moderate to moderately severe hearing loss configurations.
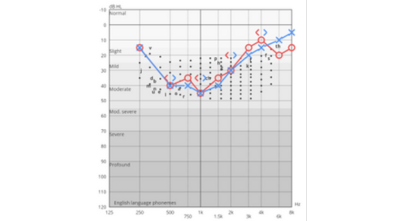
Figure 3. AutoREM is equally effective in reverse configurations, such as mild to moderate rising hearing loss approaching normal or slight thresholds.
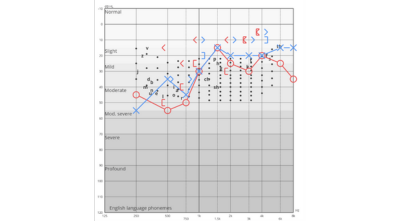
Figure 4. AutoREM can also be successfully applied in cases of moderate rising to mild hearing loss.
AudiologyOnline: Are there any audiogram configurations where AutoREM should be avoided?
Clayton Fisher: Yes, generally, the further a hearing loss deviates from the moderate range, whether toward slight/mild or toward severe/profound, the less appropriate AutoREM tends to be. Below, I’ve outlined several situations where AutoREM may not be the best choice.
AutoREM is not recommended for slight or mild hearing losses, nor for any low-gain hearing aid fittings. In these cases, prescriptive targets are often unreliable, as the patient’s average speech levels may already exceed the prescribed target, even before any amplification is applied.
Here are some examples of challenging hearing loss configurations where I would personally avoid using AutoREM:
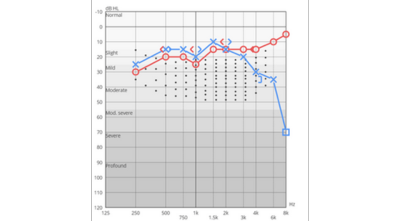
Figure 5. Asymmetrical mild high-frequency sensorineural hearing loss (SNHL): not ideal for AutoREM.
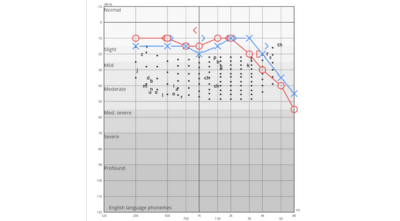
Figure 6. Mild high-frequency hearing loss: AutoREM may be unsuitable.
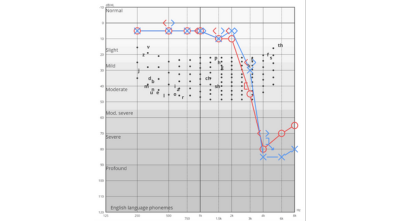
Figure 7. Steeply or precipitously sloping high-frequency hearing loss: AutoREM may not be appropriate due to a high risk of feedback. The system does not account for this and will raise gain to target regardless, potentially causing feedback issues.
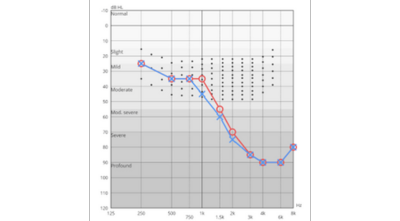
Figure 8. Another challenging hearing loss configuration where AutoREM may not be appropriate.
AudiologyOnline: Are there other differences or limitations of AutoREM compared to a manual approach?
Clayton Fisher: Yes, AutoREM does come with some limitations.
One concern I have is that many (though not all) AutoREM implementations do not display Speech Intelligibility Index (SII) values, either aided or unaided. These values are incredibly helpful in estimating a patient’s perceived benefit from amplification. For more on this, I recommend watching this webinar: Measuring and Assessing Aided Audibility Using the SII.
If you're aiming to assess how much the SII has improved with amplification, you’ll likely need to perform a few manual measurements after the AutoREM process.
Additionally, some AutoREM systems do not support maximum power output (MPO) adjustments or allow verification at multiple input levels. These steps may also need to be completed manually following the initial fitting.
That’s why I recommend using AutoREM as a strong starting point. It will get you very close to target efficiently. From there, a few quick manual adjustments can help fine-tune the fitting and ensure that the patient's perceived loudness is comfortable and appropriate.
AudiologyOnline: Besides improved accuracy and speed, are there other benefits to AutoREM?
Clayton Fisher: Absolutely. For new clinicians who may not yet feel confident performing real-ear measurements manually, AutoREM offers an excellent way to reduce potential errors and improve the quality of hearing aid fittings.
For instance, most AutoREM systems will automatically mute the hearing aids during level calibration when an open acoustic setting is selected. This prevents sound leakage from the ear canal into the reference microphone, a common cause of inaccurate measurements that less experienced clinicians might easily overlook.
In addition, some AutoREM systems include automated warning prompts when the deviation from target is unusually large. This can help identify potential problems such as a dislodged probe tube, before continuing the fitting process.
Finally, for clinicians who may not yet feel comfortable making significant manual adjustments to a patient’s hearing aid settings, AutoREM provides a safe and effective way to carry out those adjustments automatically, helping ensure a more accurate and comfortable outcome for the patient.
Summary
AutoREM is, without question, a game-changing technology—one that enables clinicians to enhance hearing aid fittings with greater accuracy, objectivity, and efficiency, while saving valuable clinical time.
For experienced clinicians, AutoREM offers a fast, convenient, and reliable method to reach prescriptive targets. It serves as an excellent starting point, after which fine-tuning and manual verification can be applied based on clinical expertise and individual patient needs.
For newer clinicians, the structured, guided nature of AutoREM lowers the barrier to performing real-ear measurements. Features such as automatic hearing aid muting during calibration help prevent common errors and foster confidence in the fitting process.
That said, AutoREM is not a replacement for clinical judgment. It’s not suitable for every patient or hearing loss configuration, nor does it eliminate the need for professional insight. Rather, it should be seen as a powerful and neutral tool, one that supports, but does not substitute, the clinician’s expertise.
If you haven’t tried it yet, now is the time. Start using AutoREM, and you’ll quickly see the difference it can make in your daily practice.
Two Complete AutoREM Examples
Below are two clinical cases where I found AutoREM to be particularly beneficial. Both fittings were performed using the Inventis Trumpet REM hardware, with AutoREM initiated through the Starkey ProFit fitting software.
First Example
In the first example, the manufacturer’s default best-fit settings were well above the target, resulting in over-amplification for the patient. AutoREM was able to significantly reduce the gain, aligning the output more closely with the prescriptive targets and improving overall comfort.
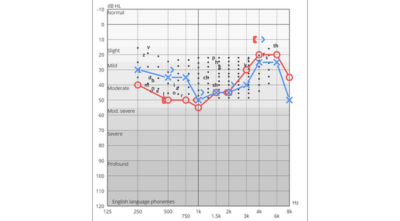
Figure 9. Pure-tone audiogram (PTA) of the patient in Example 1, used as the basis for the initial hearing aid fitting.
Step 1: Probe Tube Calibration performed prior to AutoREM measurements. (Figure 10)
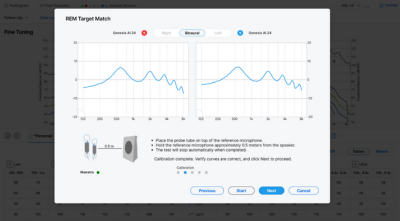
Figure 10
Step 2: Measurement of the ear canal resonance of the open ear. (Figure 11)
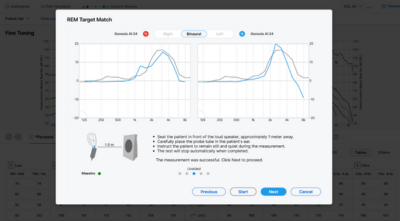
Figure 11
Step 3: Solid thin lines below show the target curves (Figure 12)
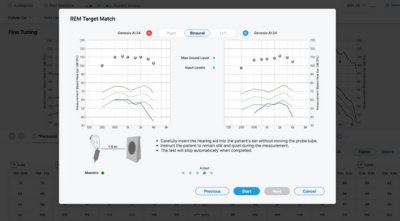
Figure 12
Step 4: Dotted lines below show the measured responses, before adjustments (Figure 13)
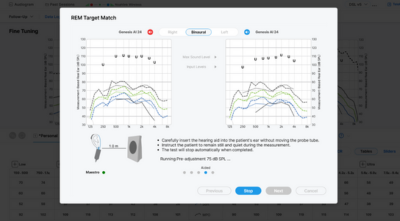
Figure 13
Step 5: The solid bold lines show the response post-adjustments (Figure 14)
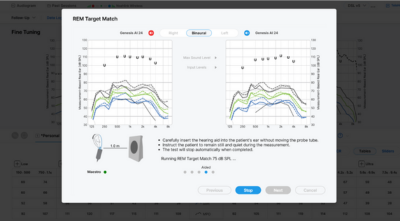
Figure 14
Final Step – Manual Verification of AutoREM Accuracy (Figure 15)
To confirm the effectiveness of the AutoREM process, I performed a manual real-ear measurement. The results showed an excellent match-to-target, with both aided and unaided SII values available for reference.
In the graph, the dotted line represents the prescriptive target, while the solid line shows the measured aided response after AutoREM adjustments were applied.
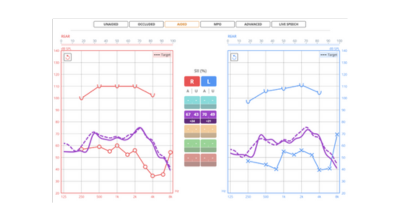
Figure 15
Second Example
In this second case, the initial best-fit provided by the manufacturer’s fitting software resulted in significant under-amplification. The output was well below target across key frequencies.
AutoREM effectively addressed this by automatically increasing the hearing aid gain, bringing the measured response much closer to the prescriptive targets and improving audibility for the patient.
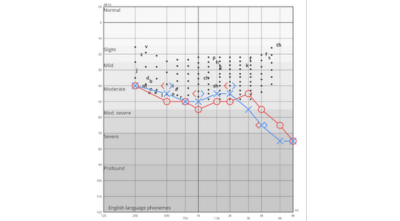
Figure 16. Pure-tone audiogram (PTA) of the patient in Example 2, used as the basis for the initial hearing aid fitting.
In this example, the graph illustrates the complete AutoREM correction process. The thin solid lines represent the prescriptive targets, while the dotted lines show the initial measured response before any adjustments were made.
Following the AutoREM procedure, the bold solid lines display the corrected aided response, now closely matching the prescribed targets (Figure 17).
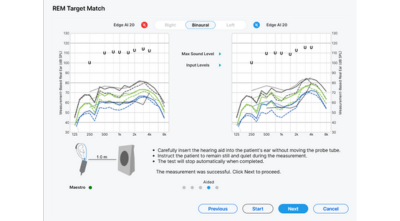
Figure 17
To confirm the effectiveness of the AutoREM correction, I performed a manual real-ear measurement.
The results demonstrate a close match-to-target, validating the accuracy of the automated fitting.
In the graph (Figure 18), the dotted line represents the prescriptive target, the solid line shows the measured aided response, and the turquoise curve below illustrates the unaided response, provided for reference.
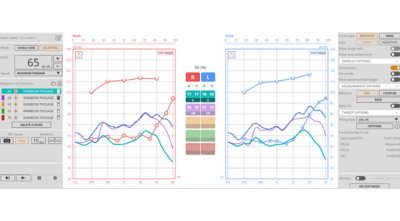
Figure 18
Resources for More Information
For more information about Inventis, visit https://www.inventis.it/en-na
Check out the following courses published on AudiologyOnline:


