
Editor’s Note: This text course is an edited transcript of a live seminar. Download supplemental course materials.
Jessica DeFauw: To get started, I would like to introduce Jennifer Henderson-Sabes. Jennifer is an audiologist at University of California – San Francisco. She is a researcher who has been published in many journals and various presentations in the areas of tinnitus management and auditory rehabilitation. As it relates to LACE and LACE Online, Jennifer is one of the co-developers of this auditory rehabilitation program. We are excited to have her here to share some information about how LACE was developed, how it works, and how we can use it as part of a well-rounded clinical protocol.
Jennifer Henderson-Sabes: As Jessica mentioned, we are going to talk about LACE - specifically, LACE Online. The focus of today’s talk is to learn about how to integrate LACE Online with Sycle. We will talk about the basics of LACE for individuals who have not used it yet. We will talk about some new LACE Online features that are available to all LACE Online users, as well as some that are specific to Sycle users. We have some data that show the benefits of both LACE and LACE Online, and we will help you understand how to use LACE Online in Sycle. If you are using it in Sycle, we will help you understand the data that you get through your Sycle interface.
By the end of today’s webinar, we hope you will understand that LACE Online can benefit your clinical practice. The benefits to each practice are different. Our goals is that you can take what we talk about, apply it to your clinic, and find the ways in which it is most helpful for you.
Integrating LACE Online with Sycle simplifies the process. Today we will talk about some of the features that are involved in LACE Online and specifically those that are implemented through Sycle. I will touch on some helpful hints for how to interpret the data, and Jessica is going to take a few moments at the end and talk about how to turn on LACE Online in Sycle and how to streamline the dispensing process so that you feel comfortable turning it on tomorrow.
LACE Online
LACE Online was developed a few years ago. It came out of research based on the conventional LACE training, which we call Home Edition (HE). There are some significant benefits for using LACE Online. First, it is a cloud-based training program. It has the same basic training as LACE HE. The training modules are very close to what is used in LACE HE, but there is no disc or download that needs to be implemented on that computer. If you use it through Sycle, there is some clinician monitoring that comes with it, and we will talk about that.
LACE Online is an 11-day program rather than a 20-day program, and we have an understanding of the benefits and the trajectory of training from the thousands of people who have already used LACE. We learned that more than 60% of the maximal benefit occurs in the first 10 days. We have lots of information about what kinds of benefits occur, and for many people, the first 10 days is where we see most of the training happening. The LACE Online training shortens the program so that it is much easier to implement into the day-to-day life of many of our patients. Although it is a shortened program, it still gives significant benefit.
With LACE Online, the individual can train anywhere with standard Internet browsers. It can be used with a tablet or a smart phone, but it does require a device with Internet access. One of the things to remember is that just because a device has Internet access does not always mean it has the best audio. Our smart phones are great for lots of things, but not listening with high-quality sound. If a laptop, tablet or smart phone is used, some inexpensive speakers or headphones that the patient can use their hearing aids would be of significant benefit.
I want to provide some background for those of you who have not used LACE or are unfamiliar with the basic components of LACE training. LACE is a home-based aural rehab program that incorporates different areas of the AR process. There are standardized assessments throughout the training. This is beneficial for both you and your patient to know how well the training is or is not transferring to a standardized assessment.
In LACE Online, one of the standardized assessments is the QuickSIN. Figure 1 shows the screenshot of what the patient would see during one of these test sessions. They will make their own judgment about how many words they understood correctly from the QuickSIN sentence. The sentences used with the QuickSIN are the Institute of Electrical and Electronics Engineers (IEEE) sentences. It is the same test, just embedded in LACE Online.
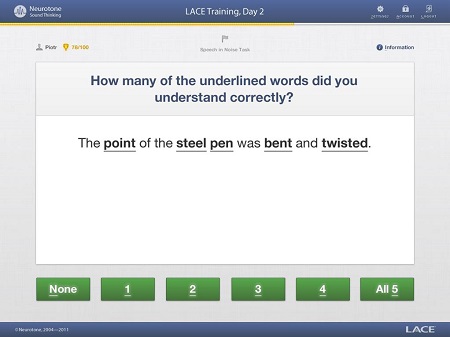
Figure 1. Screen shot from LACE Online standardized QuickSIN testing.
The user hears the sentence and is asked how many underlined words they understood. We ask them to repeat it back, and then indicate which words they got correct. They determine how many of the underlined words (Figure 1) they understood and then click on the appropriate number. This QuickSIN is scored in the same manner as the regular QuickSIN. It is presented a little differently to the patient who may not understand dB SNR (signal-to-noise ratio) loss, but you as the clinician will always have access to that data.
As well as the standardized assessments, the trainee will also have adaptive training in difficult listening environments. Throughout the training, they will be trying to hear a single speaker imbedded in babble noise. They will also attempt to hear a single speaker with a single competing speaker. There is time-compressed speech, which is termed rapid speech. It drives the individual to listen quickly, and if they become proficient, much of that content gets dropped out of the time compression. As that time-compression gets faster, they will miss more of the speech. They have to make use of many different skills to be able to perform well in this condition. The program does provide some helpful hints along the way.
Figure 2 shows a screen shot of the topics that are available during the training. The individual can select the content topic; each presentation is a sentence, and all of the content is related to that topic. If they selected Money Matters, for example, all the content during their training will be related to financial topics. They must use their cognitive skills to fill in what they are missing, based on the fact that they know that the content will be about this particular topic. They can switch topics throughout the training.
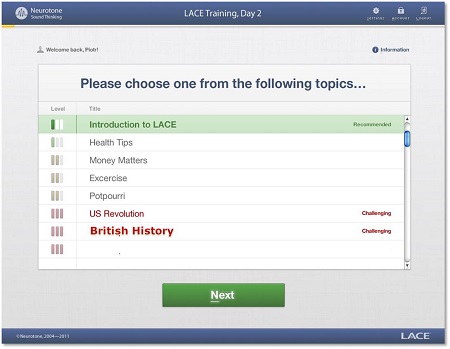
Figure 2. Screen shot of training topics in LACE Online.
Figure 3 shows a screen shot from the training where we are asking the individual to indicate whether or not they heard the sentence correctly. First, they hear the sentence and then they are allowed some time to judge what the sentence was, and then they are asked if they understood the sentence correctly. They indicate this by yes or no. If they indicate yes, then the next presentation will be more difficult. If they select no, it will be easier. In that way, they are always training near their threshold. One of the things we try to indicate to patients during the training is that it may not feel like they are getting better because they are missing the same number of questions. That is okay. We are pushing them further and further to get more and more difficult content.
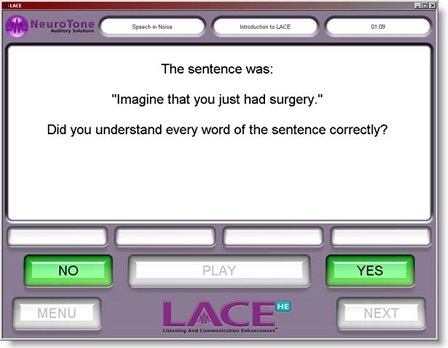
Figure 3. Screen shot during the training where the patient must indicate if the sentence was understood correctly.
Additionally throughout the training, there will be helpful hints with counseling material that you wish you could provide, but do not have the time to during your busy clinic day. This includes informational counseling about listening and communication skills, how to use hearing aids effectively, how to position oneself in an acoustic environment to have the best effect and more. All of this will be presented several times a day throughout the training, and the patients do get a lot of information about how to use their hearing aids and how to communicate effectively.
Figure 4 shows two screen shots of the communication hints. The first is reminding the individual to use vision when they can and to think about lighting. The second is reminding them that sometimes louder is not better, so they need to think about different ways that they might be able to manage their environment, such as asking the speaker to talk slowly rather than loudly.
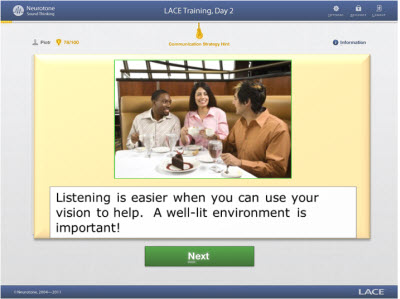
Figure 4. Examples of helpful hints that are presented throughout the LACE Online training.
Throughout the training, the individual will get feedback about their performance, because they know whether or not they understood the sentence correctly. At the end of each days’ training, they will get a score that takes into consideration where they started and where they have ended at that point, and how they are performing relative to days past. They will get some feedback about how they are doing in a way that makes sense to them. It comes by way of points, and the more points they get, the better they are doing. They have a little bit of information about how they are doing based on the number of points they get at the end of the day. Figure 5 is an example of what a user would see at the end of their training day. In the left corner, they would have the day that they trained. They would see their past days, and they would see their points. They will also see some information about their standardized assessments.
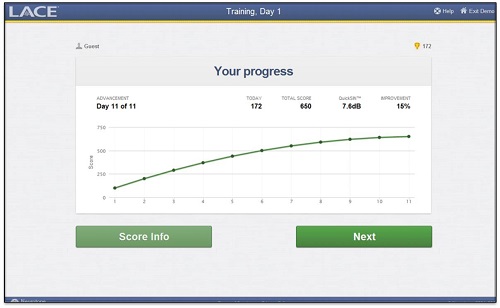
Figure 5. LACE program feedback screen.
LACE Online Features
There are new features that are exclusive to LACE Online, and some of these are even exclusive to Sycle. You can think of LACE HE as a less modular training system. LACE Online has the benefit of us being able to integrate features, try them out and see what works. We have some new features that we think are going to be helpful for the training process.
You saw some of the helpful hint screen shots, but we have also implemented several helpful hints videos to try and maintain interest and keep things vibrant throughout the training day. There are more introduction videos introducing the task and LACE training. These encouraging videos remind them to practice and implement what they are learning into their daily environment. A good portion of the communication strategies will be implemented as video. There are days where some of the communication strategies are shown through video rather than a photo with information about what they should do. One example shows walking into a theater, finding the assistive listening device, putting it on, and sitting down. Maybe they have seen the assistive listening signs before, but they are not sure how to implement it in a public place; now they see how to do it and how to position themselves in many different environments. Figure 6 shows a screen shot from one of the videos.
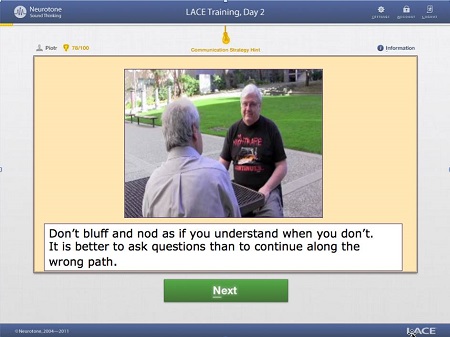
Figure 6. Screen shot of video helpful hint from LACE Online.
In this video (Figure 6), we remind people not to bluff and nod when they do not understand, as easy as that may be. What they will see in this video is two men conversing, and one is smiling and nodding. It becomes clear through the video that he would not be smiling and nodding if he knew what the content of the conversation. He gets into a situation where he needs to acknowledge that he does not understand. It is a familiar situation for many individuals, and you can somewhat successfully extricate yourself from that situation. It not only adds another dimension to the training, as a video is a welcome break when you are training, but it also allows people more insight into many of the communication strategies that they face on a regular basis.
Two additional standardized tests have been implemented exclusively to LACE Online to look at the subjective domain. We have included the Hearing Handicap Inventory for the Elderly (HHIE) where the social, emotional, and total scores are tracked. We also have the Communication Confidence Profile, which is a 12-item scale that asks the individual to provide information about their confidence and self-efficacy in a variety of different listening situations.
Figure 7 is a screen shot of the HHIE. It asks, “Does a hearing problem cause you to use the phone less often than you would like?” The patient selects yes, sometimes or no. Figure 8 shows one of the items from the Communication Confidence Profile. “Are you confident that you can understand a person speaking in a large room, like an auditorium or house of worship?” The user selects one of five buttons at the bottom of the screen.
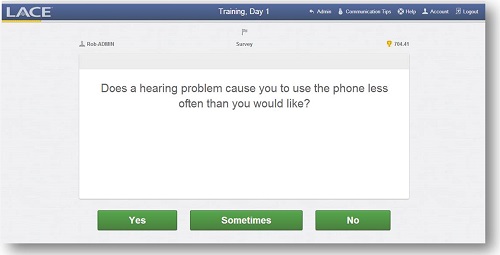
Figure 7. Screen shot of the HHIE questionnaire in LACE Online.
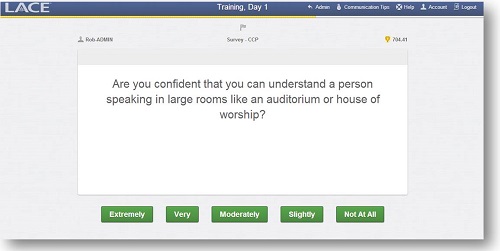
Figure 8. Screen shot of the Communication Confidence Profile in LACE Online.
With these new interfaces, we are able to obtain information about these subjective perspectives, which we have not had much access to in the past. We can get an idea of whether handicap is shifting over the course of training and whether the patient’s confidence in difficult listening situations is influenced by the training with the hearing aids in or all of the information that they get throughout the training.
The patient will get feedback about their training, and Figure 9 highlights where they will see the HHIE and Communication Confidence Profile scores when those occur throughout the training. It breaks apart the social and emotional components of the HHIE for trainees as well. When they hover the pointer on the individual scores they will get information about where they fall. They will get some information about how confident they are from the Communication Confidence Profile, as well as an indication of where they fall relative to the normative data for hearing handicap.
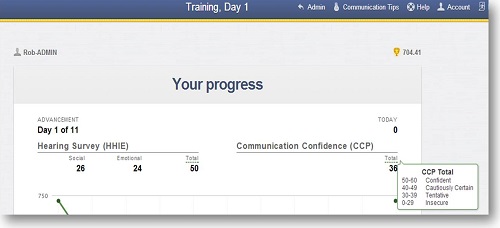
Figure 9. Screen shot showing patient progress and feedback on the HHIE in LACE Online.
Auditory Training
A good portion of what is in LACE and LACE Online is auditory training and time spent in difficult listening environments. LACE has a perspective that is very much about hearing aid users, and it is an excellent way to have individuals practice with a new set of hearing aids. Above and beyond that, there is evidence to support that auditory training is beneficial. In the last few years, we have seen evidence supporting auditory training in general (Tye-Murray, Sommers, Mauze, Schroy, Barcroft, et al., 2012; Millward, Hall, Ferguson, & Moore, 2011; Humes, Burk, Strauser, & Kinney, 2009). In fact, there was a special issue of the International Journal of Otolaryngology a few months ago that specifically addressed plasticity of the brain in adults and older adults with hearing impairment who use hearing aids.
In addition, there is published evidence specifically supporting LACE training (Song, Skoe, Banai, & Kraus, 2012; Sweetow & Henderson-Sabes, 2006), and in the past few years, we have seen an electrophysiological study come out of Northwestern University looking specifically at LACE training. There was a beta study that we did at University of California – San Francisco. There was a study looking at a few hundred patients in a large clinical practice. Olson et al. (2013) also published a study about the LACE DVD training, which we will not talk about today, but that version uses the same training components in a DVD format. It is certainly our least feature-rich version of the training, but even LACE DVD does show improvements with hearing aid users.
Implementing LACE into Your Practice
We will talk about how you can implement LACE Online in your practice, but some of the questions we often get are, “Who should do LACE? Should I give it to everyone? Should I reserve it for a specific population? How I should focus my direction on LACE?” We conducted a study a few years ago looking at whether we could predict who would get the most benefit from LACE based on their incoming scores. We looked at factors such as age, speech performance in six different tests, subjective reports and cognitive performance. Interestingly, we found that performance on any given test could not reliably predict the overall improvement. That being said, poor scores on subjective measures and speech tasks were correlated with greater improvement. Over time, we have seen that to be the case as we look at the identified data that we have for trainees.
That means that you should not rule out those individuals with more significant impairments when you are thinking about doing LACE Online training. In fact, patients of all skill sets will show some knowledge improvement with the helpful hints that we are talking about. When we are talking about improvements to speech perception, those with the most significant impairments will show the greatest improvement. We encourage you to put LACE out there for all of your patients, even those with poor speech understanding. One thing to remember is that LACE is adaptive, so the easiest level is essentially speech in quiet. You can think of it as being appropriate for many individuals regardless of their incoming performance.
Benefits
About a year and a half ago, we took all of this data from our trainees to see if our understanding, based on a clinical study, held true in the real world. We looked at baseline QuickSIN scores for all the individuals who completed the training. Then we looked at their final QuickSIN score at the end of the training, and we compared the two scores to determine improvement. Figure 10 shows the magnitude of improvements. The X-axis is the baseline QuickSIN score. The dotted lines running vertically indicate the separation between normal, near normal, SNR loss mild, SNR loss moderate, and SNR loss severe. The Y-axis is improvement in the QuickSIN score. You will notice that the individuals who had essentially normal QuickSIN scores did show clinically significant improvement on the QuickSIN, but if you compare that group to the group who had a moderate SNR score, you will see that the moderate group had an even greater improvement on the QuickSIN score. Obviously, the normal and near-normal groups had some ceiling effects that we cannot alter, but I wanted you to see that the changes between the baseline QuickSIN scores and the magnitude of improvements. In our severe group, you can see that there are still improvements for those with greater than 15.5 dB SNR loss. For those who cannot get a single word on the entire QuickSIN, they do improve, but the absolute improvement starts to diminish.
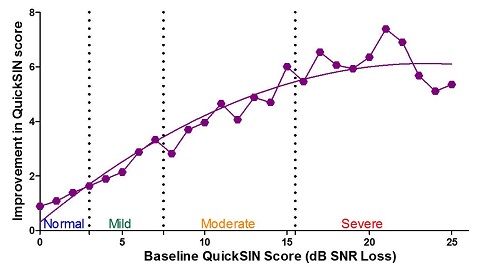
Figure 10. Magnitude of improvements on the QuickSIN relative to the baseline QuickSIN score, or amount of SNR loss.
Given that information, we looked at normative improvement for each of these groups. Keep in mind that our moderately to severely impaired individuals, in terms of speech performance, might be good candidates for LACE. We are seeing anywhere from a 1 to 6 dB improvement relative to the normative data. Know that 1 dB improvement in SNR has been estimated to be the equivalent of about a 6% to 8% in percent-correct scores for sentence recognition (Crandell, 1991). We are hopefully providing them with the skills to go out into the world and have improved speech understanding.
There are other benefits to using LACE. We have seen some independent studies examining the clinical usage of LACE and hearing aid use. The studies tend to look at return for credit. Martin (2007) looked at many clinics within one practice. They went from a 13% return-for-credit rate to a 3.5% rate by simply implementing conventional LACE. Brian Taylor and Al Shrive (2008) looked at the integration of nine in-office sessions of LACE Clinic Edition (CE). Some clinics opt to have individuals come in and do LACE training. The nine in-office sessions are roughly equivalent to LACE Online’s number of training sessions. From that study (Taylor & Shrive, 2008), we saw a 15% return-for-credit rate diminish to 3% for those individuals who did the LACE training.
Another study used 23 clinics to examine 541 fittings in a six-month period. They provided LACE similarly to different patients. There were 294 patients that did not receive LACE and 241 that did. There were 58 returns in six months from the entire group; 44 were non-LACE patients, which calculated to approximately a 15% return-for- credit rate, and only 14 of those returns were from individuals who did use LACE.
In a 10-clinic study, over 523 patients did not receive LACE and 170 did. In this particular study, they looked at average return rate, but they included exchanges as “returns” as well. In this study, there was a 28% return rate, including exchanges, for those who did not use LACE, and a 5.3% return rate for those who did receive LACE. Furthermore, the researchers broke down the LACE compliance for each of the 170 patients in order to find out the particular return rate as the number of completed LACE sessions increased. We know that not everyone finishes LACE. They looked at how much of the LACE training the individual completed. They did not ask the individual how much training they did, which is an important factor.
Sixty-seven of those patients did 11 or more LACE sessions, and their return rate was 4.5%. Forty-three did more than 1 but less than 11 LACE sessions, and their return rate was 4.7%, which was no different than the previous group. What was interesting was that 60 of the 170 patients came up as not completing a single session. They logged in, but it looked like they had not completed a single session. That group had a return rate of 6.8%. By looking at this, it seems like just handing LACE to someone or telling them that they should do it would affect their return rate. We do not think that that is absolutely the case, although you could make a case for that. Some portion of these patients indicated that they did not want their clinician to follow them through their training, so the clinician could only see that they registered, but not how many LACE sessions they completed. That said, it is interesting that the possibility of mentioning that LACE is important can have an impact on return rate.
Sycle implemented LACE Online over one year ago. They have since looked at about 400 users who completed the 11 days of LACE Online training through Sycle.net. Of those 400 users, 6 returned their hearing aids. That is a return rate of 1.5%, which is impressive, considering that the industry standard is 16%. They also looked at average visits within 90 days. They saw that when the group had LACE training, the average number of visits over 90 days was 4, and in the group that did not have LACE, there were an average of 7 visits. This kind of information is evolving, and there will likely be more like this in the coming months. The initial data looks promising and leads us to believe that the integration of LACE Online through Sycle could be a significant benefit to the average clinic.
In addition to the benefits that come with auditory training and information about how to use hearing aids and utilize good communication strategies, we hope that we are implementing better hearing aid use with more individuals, having fewer return visits, and educating patients on their active role in the rehabilitation process.
Sycle Integration of LACE Online
Jessica DeFauw: I think it is easy to see the documentation supporting the efficacy of LACE in clinical practice. I am not a researcher, but if I were still practicing in a clinic, the reduction in follow-up visits return rates alone would make me think that providing LACE and explaining it to patients would be a beneficial scenario. It helps patients take a little more ownership of the adoption of amplification and understand that they have a bigger part in that process than just daily maintenance and use of the hearing aids.
At Sycle, we are constantly looking for ways that we can make our customers' practices more efficient and profitable. We get requests from all kinds of vendors inside and outside the hearing care industry wanting to integrate with us. We have to be selective with whom we integrate, but when we started talking with Neurotone about LACE, it seemed to be a natural fit. Both LACE Online and Sycle are web-based, but also, we hear consistently that practices want to implement some type of aural rehabilitation program. They may not have the time or the resources to provide aurah rehabiliation, or they are worried that people would not take advantage of it. Integrating LACE with Sycle addresses many of those issues. It is an easy way of implementing auditory training within your practice, and it also gives you the ability to track patient compliance.
We integrated a little over a year ago and have recently made some important updates, specifically to the type of training data that is visible within the patient record in Sycle. I am going to show you some screen shots of that, and then I am also going to show you how we have streamlined the process for dispensing LACE. When you decide that it is time for a patient to start using LACE, it is very easy to generate the individual user code for them and give them the instructions.
Dispensing LACE
Dispensing LACE to patients is a three-step process. First, you will select the patient record in Sycle and then scroll to a section called Auditory Training Powered by LACE (Figure 11). When you click on the link, it will take you to a Sycle purchase summary (Figure 12). Once there, you will see a button for LACE instructions. The purchase summary provides the online access code for LACE. You can set up the price that you want to charge for LACE in the administration section of Sycle. We have seen all varieties of pricing strategies from the practices that have implemented LACE Online so far. Some practices decide to offer it complimentary to their patients as a value-added service along with hearing aid purchase, which, given the return for credit rate data, seems to make sense. It might be in the best interest of the practice and the patient to provide it at no charge. Some practices decide to use it as another opportunity for revenue and offer it at a set fee per patient. The sample in Figure 12 charges $50. It is up to you as the practice and provider to decide what you want to charge.

Figure 11. Example of where to access LACE within the patient record in Sycle.
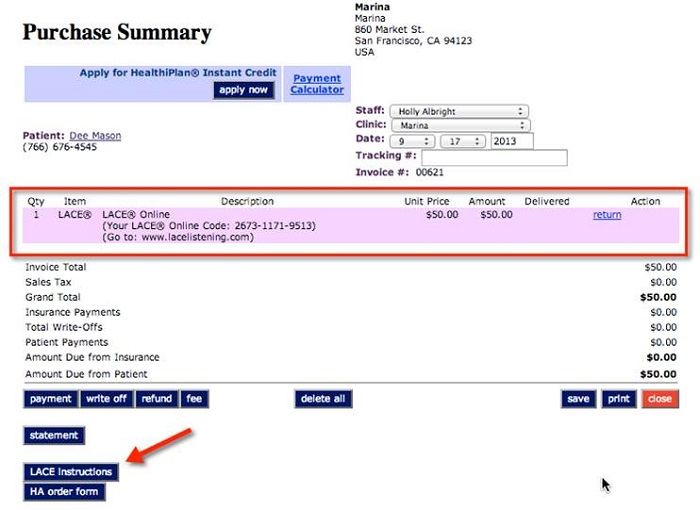
Figure 12. Example of purchase summary screen in Sycle.
Once you have added LACE to the purchase summary, click on the LACE Instructions button at the bottom of the page. It will give you a detailed PDF document that will provide the patient the information that they need in order to get started with LACE, as well as where they need to go to enter their access code (Figure 13). It automatically populates the patient name and the access code that comes directly from Neurotone. They log into LACEListening.com, enter the access code, and then can proceed with their training. It also gives some recommendations regarding best practices with LACE. It shows the patient what they need to know about getting started, and then offers them contact information in case they run into any challenges or need technical support.
Figure 13. Example of LACE patient document that provides instructions and access code for the training.
After you have discussed the importance of LACE with the patient, all you need to do is print the PDF form. The majority of our practices who are currently using LACE give the patient the information, and they take it home to log in on their own. I have spoken with one or two practices that have a dedicated workstation set up in their office. Patients can come to the office, log in to LACEListening.com, and use their access code there. That is an option to get patients back in to the practice, or for patients that need access to a computer.
We also added some more detailed information within the patient summary. You now can see the patient’s test scores and the number of the training sessions that they have completed. Figure 14 shows the same patient summary screen, but now you can see that once the patient has started LACE, you are shown additional information about their training program. Each day, we automatically get that information from LACE and update it in the patient summary. You can look any time and see how your patient is doing. For example, you can see how their scores are improving on the QuickSIN, speech in noise, and rapid speech, et cetera. If you hover over any of the question marks next to the test category columns (Figure 14), it will give you an explanation of what score you are looking at and provide a link for additional information about how to interpret those scores. You can add notes at the bottom of the page. You now have comprehensive information about how that patient is doing with their training program.
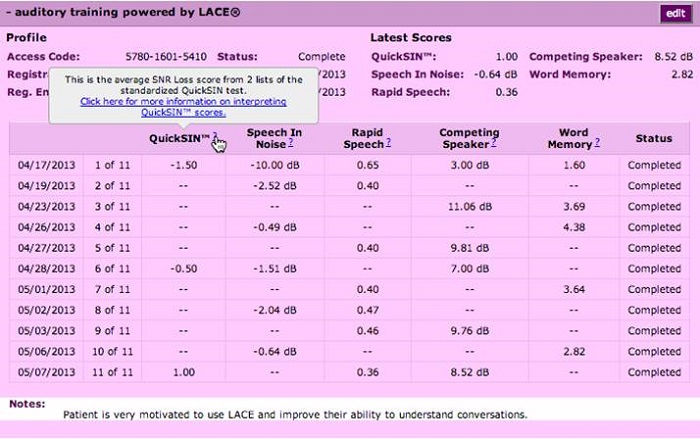
Figure 14. Patient summary screen with imported LACE training results. Hovering on the question marks in the test column provides information on interpretation of the test.
Let’s say they have completed one or two sessions, and then a week or two goes by and you do not see anything else. That might be a time to pick up the phone and call to see how things are going, particularly if they are in the trial period with their hearing aids. It gives you a window into whether or not they are complying with the program, and that opens an opportunity for you to have a conversation with the patient about it as you feel necessary.
Pricing
As I mentioned, you have several different options to how you would implement the pricing piece of LACE within your practice. We wanted to make it easy to accommodate all of those different scenarios. What we offer through Sycle is an unlimited rate. No matter how many LACE access codes you generate or how many patients access the program, it is $119 per month for a full-time clinic and $69 per month for a part-time clinic. As a point of comparison, the wholesale price directly through LACE is $200 for 10 access codes. I think the unlimited codes through Sycle for $119 a month is a great deal. Also for your information, if a patient were to go directly to LACEListening.com and purchase LACE Online for themselves, it is $79.
If you are interested in getting started with LACE or would like an overview of what the patient will experience, you can view a demo at LACEListening.com/demo. We have the enrollment for LACE Online setup within the administration section of Sycle (Figure 15). Under this section, there is a LACE Online configuration listed in the left-hand column. If you click on that, you can see it lists all the clinics that you have active with Sycle, and you have the option of adding and offering LACE through any clinic (Figure 16). Another feature in this screen is LACE Online alerts. If you turn those on, you will get an alert when you pull up a LACE patient’s patient summary; it will let you know how long it has been since they have logged in. You can also set that to only notify after a patient has been inactive for seven days, so that you are not getting constant alerts. It pops up an alert only when you pull up that patient summary. This gives you a notification that the patient has stalled in their training and provides you the ability to reach out. There is a specific report in the Reports section of Sycle that lists all the patients who are in process of LACE training at any given time.
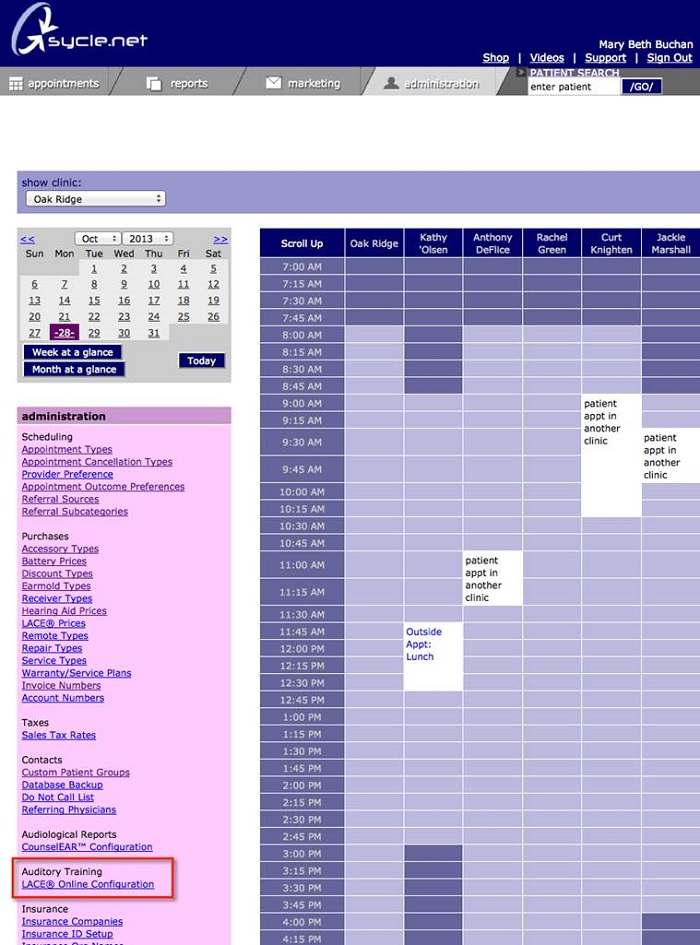
Figure 15. Administration section of Sycle. LACE Online configuration can be found on the left-hand column.
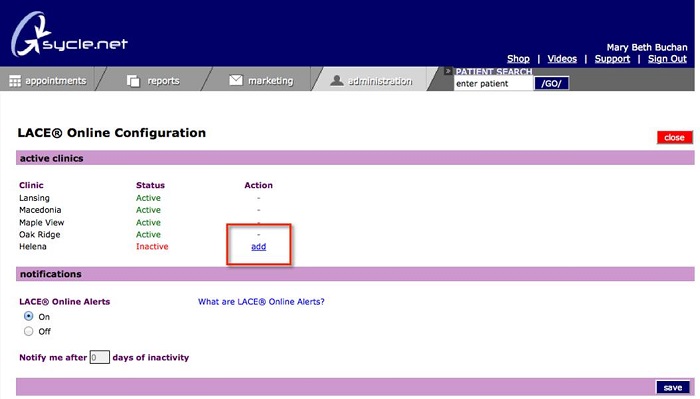
Figure 16. LACE Online configuration screen, showing active and inactive LACE clinics.
If you are interested in any more information about Neurotone or about LACE, you can visit www.neurotonepro.com or www.lacelistening.com. You can also e-mail information@neurotone.com with any questions. As always, you can call Sycle anytime at 888-881-7925. Our account reps that answer the phone are all well-versed in how LACE works.
Question and Answer
Is the fee per location or per practice?
It is per location. If you have two full-time locations within your practice, it would be $119 per month, per location. If you are interested in doing a test run, you can start by offering it from one location first. You do have the option of selecting at which locations you would like to offer it. It does not have to be an all-or-nothing proposition.
How long is the typical LACE session?
The typical LACE session is 20 to 30 minutes, depending on the patient.
I am new to LACE and earlier this year, I had a patient use the online version at home. She reported back to me that she received a score of 0% improvement. Is this possible, and how do you recommend proceeding with her?
It is possible to not have any improvement over the course of the online version. That typically happens when they are looking at QuickSIN scores. If they did not improve on the QuickSIN, then they would have a score of 0% improvement. Generally speaking, they will see improvement points on the training scores, but percent improvement is relative to the QuickSIN. These are average scores, so there are obviously people who do not get better.
As far as how to handle those individuals who do not get better on the QuickSIN, you could look at the subjective scores. If she was using the online version earlier this year, she would not have seen those. You could also talk to her about whether or not she felt more confident or whether there were benefits outside of the standardized assessment that she had. That is how we recommend approaching that. Not everyone does improve on the standardized test. Try to bring out what other benefits she received, if any.
Does LACE supply any printed materials for patients, such as informational brochures?
Yes. Neurotone does supply printed materials. You can contact Becky or Bill at Neurotone for more information.
Can the program be repeated by the patient, or is it a one-time only access?
For LACE Online, users do finish at 11 days, but at the end of 11 days, they have the option to transition to LACE HE if they would like. LACE HE is a longer training since they can select the content. There is likely some content in the home version that they did not finish in the LACE Online. With LACE HE, they can continue on for as long as they have content, up to 500 days.
If the patient transitions to the home edition, do they have to pay an additional price?
Yes they do. The price is $99 if they transition from LACE Online to LACE HE.
What is the relationship between the days of inactivity and the improvement in LACE?
We are starting to analyze that information. In some of the constrained studies, we saw that it was the earlier days of training that needed to be consistent, and those later days of training could be more sporadic. Based on the data that we have now, we would encourage users to get going consistently during that first week, but you do not have to be such a task master for the end of the training. There is a relationship between going several days between training, particularly in that first week, and less desirable outcomes.
Does the patient see their progress scores as they go along or only at the end?
They do see their scores as they go along. At the end of each day, they will get a summary about how they are doing.
Are there 500 sessions in the home version?
LACE HE has 500 days to complete training, but they do not have 500 sessions. It is 20 sessions of reported training, where they get feedback and feedback to the clinician if they want it. If they finish 20 days of training and they want to continue to train, they can do that for up to 500 days.
Do you have to utilize Sycle’s billing in order to offer the LACE access codes?
If you sign up through Sycle, you have unlimited LACE access codes. You do have the option to purchase codes in a package, 10 codes for $200 directly from Neurotone, if you wanted to do that instead of signing up on the monthly basis through Sycle.
How do you charge the patient for the training?
You go from the patient summary to the purchase summary, and you do have to add LACE to a purchase summary in order to generate the code. You can add it as a $0 item, and you do not ever have to show the patient the invoice or charge them for it all if you so choose. In terms of the workflow, it is added to a patient summary, which is nice because you can know how many patients have signed up for LACE in your total sales report within Sycle.
References
Crandell, C. C. (1991). Individual differences in speech recognition ability: implications for hearing aid selection. Ear and Hearing, 12(6 Suppl), 100S-108S.
Humes, L. E., Burk, M. H., Strauser, L. E., & Kinney, D. L. (2009). Development and efficacy of frequent-word auditory training protocol for older adults with impaired hearing. Ear and Hearing, 30(5), 613-627. doi: 10.1097/AUD.0b013e3181b00d90.
Martin, M. (2007). Software-based auditory training program found to reduce hearing aid return rate. The Hearing Journal, 60(8), 32-35.
Millward, K. E., Hall, R. L., Ferguson, M. A., & Moore, D. R. (2011). Training speech-in-noise perception in mainstream school children. Internal Journal of Pediatric Otorhinolaryngology, 75(11), 1408-1417. doi: 10.1016/j.ijporl.2011.08.003.
Olson, A. D., Preminger, J. E., & Shinn, J. B. (2013). The effect of LACE DVD training in new and experienced hearing aid users. Journal of the American Academy of Audiology, 24(3), 214-230. doi: 10.3766/jaaa.24.3.7.
Song, J. H., Skoe, E., Banai, K., & Kraus, N. (2012). Training to improve hearing speech in noise: biological mechanisms. Cerebral Cortex, 22(5), 1180-1190. doi: 10.1093/cercor/bhr196.
Sweetow, R. W., & Henderson-Sabes, J. (2006). The need for and development of an adaptive listening and communication enhancement (LACE) program. Journal of the American Academy of Audiology, 17(8), 538-558.
Taylor, B., & Shrive, A. (2008, July). The economics of computer-based auditory training. AudiologyOnline, Article 915. Retrieved from https://www.audiologyonline.com
Tye-Murray, N., Sommers, M. S., Mauze, E., Schroy, C., Barcroft, J., & Spehar, B. (2012). Using patient perceptions of relative benefit and enjoyment to assess auditory training. Journal of the American Academy of Audiology, 23(8), 623-634. doi: 10.3766/jaaa.23.8.7.
Cite this content as:
Henderson Sabes, J., & DeFauw, J. (2014, January). Using the new LACE online features in Sycle. AudiologyOnline, Article 12341. Retrieved from: https://www.audiologyonline.com


