
Introduction
Tinnitus Retraining Therapy (TRT) is a well-known, well-documented tinnitus therapy based on the neurophysiological model proposed by Jastreboff in 1990. Its main components are directive counseling to decrease tinnitus-related negative reactions and sound therapy to reduce the strength of the perceived tinnitus signal (Jastreboff, 2011). Broadband noise or conventional hearing aid amplification are commonly used in sound therapy in a TRT framework, since they are relatively neutral to listen to and thus unlikely to attract attention and induce strong emotional reactions in the patients. Music, on the other hand, is generally not recommended, since it may induce strong emotions, and may attract attention as well (Jastreboff & Hazell, 2004). However, we have seen a number of clinical cases in which neither of the two conventional TRT sound stimuli produced the desired effect. This prompted us to investigate the potential use of fractal music in TRT. Fractal music is described as sequences of tones with no lyrics, which sound something like wind chimes. Predictable without being monotonous, the music sounds familiar, but is not associated directly with music that the listener holds in memory (Sweetow & Jeppesen, 2012). It has been used in previous research with tinnitus patients (Sweetow & Henderson, 2010; Hertzfeld & Kuk, 2011; Kuk, Peeters, & Lau, 2010) with positive results.
A small-scale investigation involving 24 patients assigned to TRT categories 1 and 2 was initially conducted at the Nagoya City University Hospital, the Kasugai City Hospital, and the Sekiya ENT clinic from November 2010 to March 2011. TRT patient categories 1 and 2 have been defined as “Tinnitus a significant problem. No significant problem with hearing loss” and “Tinnitus a significant problem. Hearing loss a significant problem”, respectively (Henry, Truen, Robb, & Jastreboff, 2007).
This first study was conducted to obtain a first impression of the usability of fractal music. The results were positive, so a larger trial with a total of 91 patients in TRT categories 1 and 2 was initiated. This article reports our general findings from this trial and discusses the useful application of fractal music, based on two individual cases.
Subjects
The initial pool of subjects comprised 91 tinnitus patients (39 males, 52 females, mean age: 65.5 years ) who visited the Nagoya City University Hospital, Kasugai City Hospital, and Sekiya ENT clinic for tinnitus treatment in the period from December 2010 to February 2012. Client tinnitus history and hearing loss profile were obtained prior to the trial, and subjective tinnitus and hearing loss severity were assessed by means of the Tinnitus Handicap Inventory (THI) (Newman, Jacobson, & Spitzer, 1996; Newman, Sandridge, & Jacobson, 1998) and Visual-Analog Scales (VAS) (intensity level and frequency of occurrence), and the Hearing Handicap Inventory for Adults (HHIA) (Newman et al., 1990) scales, respectively. The Tinnitus Handicap Inventory (THI) is a 25-item questionnaire with three subscales: functional, emotional and catastrophic responses. The questions can be answered with “Yes” (4 points), “Sometimes” (2 points) or “No” (0 points). The responses are summed with a total score that ranges from 0 to 100 (higher scores indicating a greater self-perceived handicap).
The minimum THI score considered clinically significant is 18. The interpretation of the scores is (Newman et al., 1998):
0 – 16 Slight handicap
18 – 36 Mild handicap
38 – 56 Moderate handicap
58 – 100 Severe handicap
The Hearing Handicap Inventory for Adults (HHIA; Newman, Weinstein, Jacobson, & Hug, 1990) is a 25-item questionnaire with two subscales: emotional and social/situational. The scoring system for the HHIA is identical to the THI, in that “Yes” is awarded 4 points; “Sometimes” 2 points; and “No” 0 points. Possible total scores for the HHIA range from 0 to 100. The interpretation of the score is:
0-16 No handicap
17-42 Mild to moderate handicap
43-100 Significant handicap
Tinnitus was the primary motivation for seeking treatment, but many of the patients also had sufficient hearing loss to warrant amplification. The average age, gender, hearing level, THI, and HHIA scores at the initiation of the study are shown in Table 1. The average hearing level has been calculated on the basis of the pure tone audiometry as HLave = (HL500Hz + HL1kHz + HL2kHz + HL4kHz)/4.
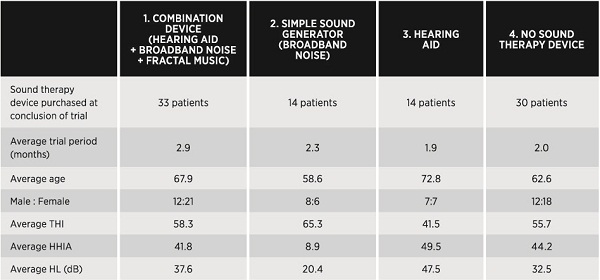
Table 1. Average age, gender, hearing level, THI, and HHIA scores at the initiation of the study, divided according to preferred sound therapy device at the conclusion of the trial.
Method
Standard TRT counseling was administered to the patients in accordance with the clinical guidelines outlined in the TRT directive counseling protocol (Henry et al., 2007). Patients trialed a sound therapy combination device for a period of 1-3 months before making a final decision on a sound therapy device purchase.
Widex CLEAR (15 channel device), Widex mind440 (15 channel device), and mind220 (5 channel device) hearing aids were selected for the trial period because they offer an optional listening program with fractal music and broadband noise (“Zen”). According to the manufacturer’s specifications, the fractal music produced in the Zen program consists of sequences of tones with no lyrics. Sounding something like wind chimes, it is somewhat predictable without being monotonous (Widex A/S, 2012). This meets the basic requirements of the TRT sound therapy protocol. The fractal music and broadband options can be used separately or in combination, with the hearing aid microphones switched on or off. Patients were given a broadband and a Zen option in the device. In addition, the default “Master” listening program, which is a conventional amplification program, was included in the device. Patients were instructed to try all options (fractal music style, broadband noise, conventional amplification) included in their devices at home. In each patient’s case it was ensured that the sound stimuli were heard in such a way that the tinnitus was only partially masked, thereby facilitating habituation in accordance with the principles of TRT (Jastreboff, 2011; Jasteboff & Hazell, 2004). The data logging function was activated to record the patients’ daily hearing aid usage and use of different program options. Re-evaluation took place after a period of three and six months, respectively. Patients also completed a questionnaire on their satisfaction with the sound therapy device after six months’ use.
General Results
As may be seen in Table 1, after the trial period 33 patients (36.3%) chose to purchase the combination device, 14 patients (15.4%) chose a simple wearable sound generator (broadband noise only), 14 patients (15.4%) opted for a standard hearing aid, while 30 patients (32.9%) chose not to purchase any sound therapy device.
The relationship between choice of sound therapy device and patient profile was analyzed subsequent to the trial. The following trend was observed:
Patients who chose to purchase the conventional simple sound generator (Group 2) were typically the ones with a relatively mild (or no) degree of hearing loss (self-perceived and objectively measured), while their THI score suggested a severe degree of tinnitus (Table 1). For these patients, the tinnitus is expected to have a greater impact on their daily lives than the hearing loss.
The reverse client profile was observed in the group who preferred conventional hearing aid amplification as sound therapy (Group 3). These patients typically had a moderate-moderately severe degree of hearing loss (self-perceived and objectively measured), while their tinnitus was at the moderate end of the scale. Thus, the assumption was that the hearing loss may be the greater problem for the patients who chose a conventional hearing aid.
Client profiles for the patients who chose the combination device (Group 1) varied, but they typically had a severe degree of tinnitus combined with a moderate (or more severe) degree of hearing loss (self-perceived and objectively measured), and a severe degree of depression. The tinnitus is expected to be perceived as more significant than the hearing loss by this group, although the hearing loss is also likely to impact their daily lives.
Reasons for not purchasing a sound therapy device (Group 4) varied, but 27% (8 patients) stated that they preferred to use their own personal audio devices (e.g., an MP3 player). 20% (6 patients) replied that they already owned a pair of hearing aids, while 17% (5 patients) were unable to perceive an effect from the sound therapy. Details of the patients’ motivation for not purchasing a sound therapy device are listed in Table 2.
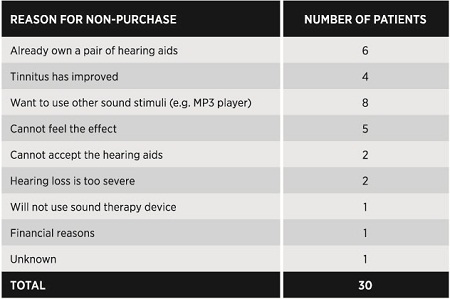
Table 2. The patients’ reasons for choosing not to purchase a sound therapy device after the trial period.
Results for Patients who used Fractal Music as Sound Therapy
Of special interest are the results obtained for the patients who used fractal music in their sound therapy (Group 1). The remainder of this paper will report the results for this specific group.
Of the 33 patients who purchased a combination device with the Zen feature, 25 participated in the re-evaluation after three and six months of therapy. Notable improvements were observed already after the first three months in the THI (Tinnitus Handicap Inventory) scores of the majority of patients who used fractal music as sound therapy. An improvement was measured in 89% of the patients after three months. 58% of these improvements were significant (20 points or more on the THI scale). After six months, an improvement was measured in 92% of the patients. 62% of these were significant. The average THI of this group fell from 58.3 at the initial visit to 30.1 after three months, and to a further 28.0 after six months. The individual THI scores at the initial visit vs. after six months are plotted in Figure 1.
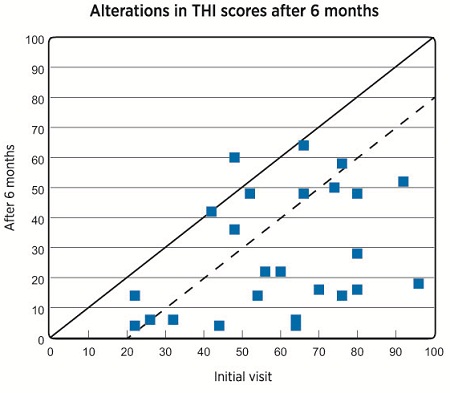
Figure 1. Scatter plots of 25 patients’ THI scores at the initial visit and after six months of therapy. Each data point represents a single patient’s THI at the initial visit (horizontal axis) and after six months of therapy (vertical axis). Data points located to the right of the stippled line indicate an improvement of 20 points or more in THI.
The patients were also asked to indicate the intensity level and frequency of occurrence of their tinnitus at the initial visit and after 6 months of therapy. This was done by means of a visual analog scale (VAS) from 0 to 100, where 0 represented no tinnitus present and 100 an unbearable level of intensity/constantly present. Notable improvements were observed both in the VAS scores assigned for intensity level and for frequency of occurrence after 6 months of therapy. The average VAS score for loudness level decreased from 72 to 41.4, and the average VAS score for frequency of occurrence decreased from 96.1 to 64.4. Individual scores (n=22 and n=23, respectively) are shown in Figures 2-3.
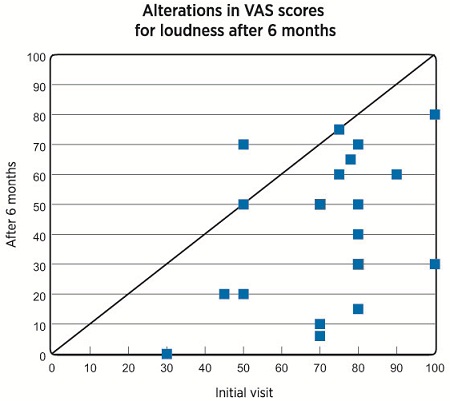
Figure 2. Scatter plots of 22 patients’ VAS scores for perceived intensity level of their tinnitus at the initial visit and after six months of therapy. Each data point represents a single patient’s VAS score at the initial visit (vertical axis) and after six months of therapy (horizontal axis). Note that some data points are hidden by identical data points (80-30: 3 patients, 70-50: 2 patients).
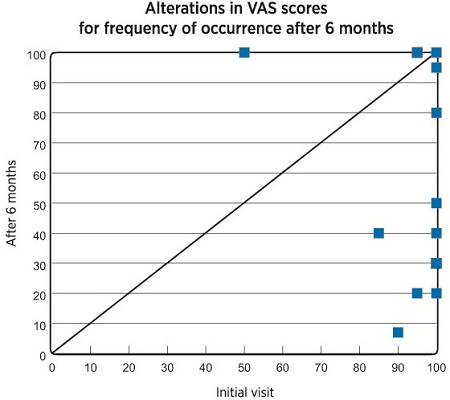
Figure 3. Scatter plots of 23 patients’ VAS scores for frequency of occurrence of their tinnitus at the initial visit and after six months of therapy. Each data point represents a single patient’s VAS score at the initial visit (vertical axis) and after six months of therapy (horizontal axis). Note that some data points are hidden by identical data points (100-30: 3 patients, 100-40: 2 patients, 100-50: 3 patients, 100-100: 6 patients).
The patients also answered a number of questions pertaining to their satisfaction with the sound therapy device after six months. The results are summarized in Figures 4-8.
Overall satisfaction scores are shown in Figure 4. 69% of the patients reported being either satisfied or very satisfied with the sound therapy. A small minority (8%) reported being dissatisfied, while 23% replied that they were neither satisfied nor dissatisfied with the therapy.
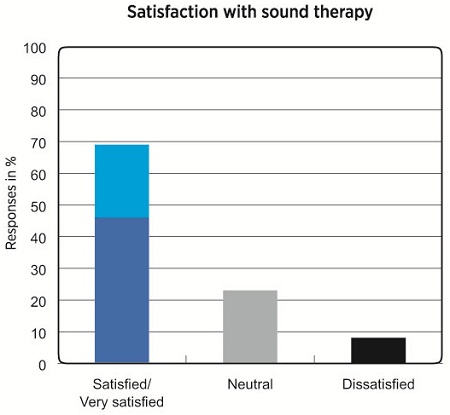
Figure 4. Overall satisfaction with sound therapy in patients who used Zen for 6 months.
One of the basic rules for the use of sound generators in successful TRT treatment is that it must not evoke negative feelings in the form of discomfort or annoyance in the patient (Jastreboff, 2011). The patients were therefore asked to evaluate the fractal music in terms of how pleasant they perceived it to be, and whether they had become tired of it after six months’ use. 65% reported perceiving the fractal music as either comfortable or very comfortable, while 35% were neutral. None of the patients reported perceiving the fractal music as uncomfortable to listen to (Figure 5). However, approximately half of the patients indicated that they had grown tired of the music after six months’ use (Figure 6).
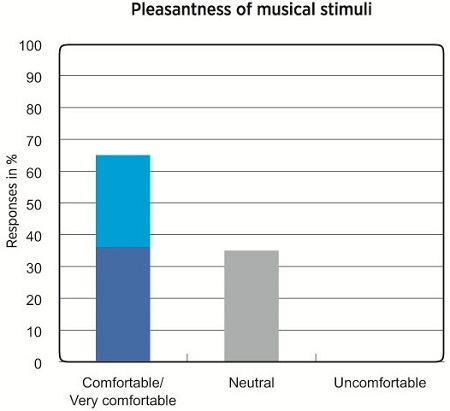
Figure 5. Pleasantness of fractal music after six months of use.
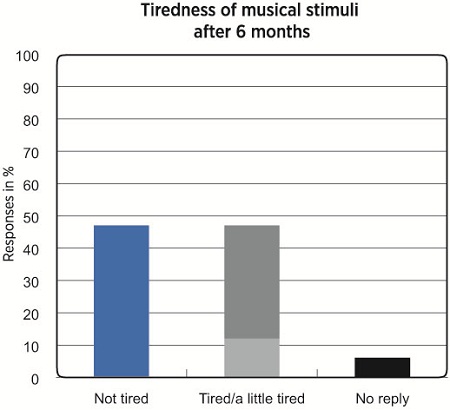
Figure 6. Tiredness of fractal music after six months of use.
Of interest was also whether the fractal music would interfere with the patients’ speech perception. According to the manufacturer, under normal circumstances the music should not interfere with speech perception, unless the patient has a very narrow dynamic range resulting from a severe degree of hearing loss (Widex zen therapy, 2012). This was largely supported by the results in the present study, as 82% of the patients reported being able to hear speech well in the presence of fractal music (see Figure 7).
Affordable price was reported to be the main motivation for choosing a simple broadband sound generator by many patients in Group 2. Patients in Group 1 were therefore asked to evaluate the combination device in terms of price. 75% of the patients who had chosen the combination device responded that it was expensive, 8% that it was too expensive, while 13% found it reasonable.
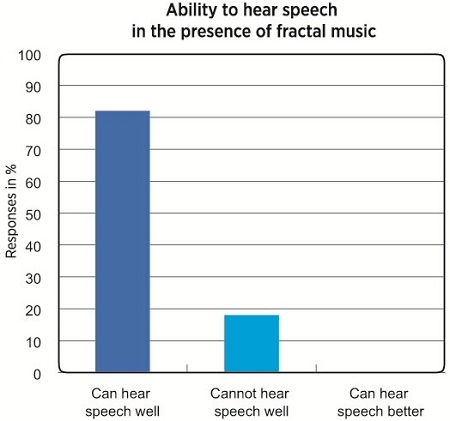
Figure 7. Self-perceived ability to hear speech in the presence of fractal music.
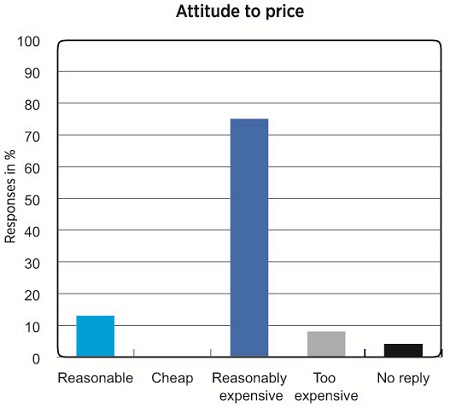
Figure 8. Patients’ attitude to the cost of the combination device.
Successful Use of Fractal Music in TRT: Two Case Reports
The following two case studies illustrate how fractal music can be useful as a sound therapy option within a TRT framework. Both cases were part of the initial pilot study group of 24 patients.
Case 1
Case 1 was a 70-year-old female who had had severe hearing loss in her left ear since childhood. At her initial visit, she was diagnosed with sensorineural hearing loss with an average hearing level of 38.8 dB at the right ear, and 76.3 dB at the left ear (Figure 9). She was not concerned about her hearing loss, however, and had not considered hearing aids. Her motivation for seeking help was a strong perception of tinnitus in her right ear which had begun two months previously and had steadily grown worse. She assumed her tinnitus was triggered by fatigue. The tinnitus had a pervasive negative affect on her daily life, making it difficult for her to maintain her relationship with her family, and reducing both her performance at work and her ability to do simple housework at home. Her appetite was lost from anxiety and fear that the tinnitus would remain untreatable until her death. Prior to her visit at the Sekiya ENT clinic, she had sought treatment in several other clinics, and had tried a variety of therapies, but had experienced no improvement. She had also tried psychiatric therapy, but to no avail. Her THI score was measured at 96 and her HHIA score was measured at 54. Visual Analog Scale (VAS) measures of 100% were assigned by the patient for both loudness and frequency of occurrence of the tinnitus. The patient’s level of depression was also assessed using the Hospital Anxiety & Depression Scale (HADS) (Zigmond & Snaith, 1983). This indicated that the patient suffered from severe depression (14/21 for depression and 16/21 for anxiety).
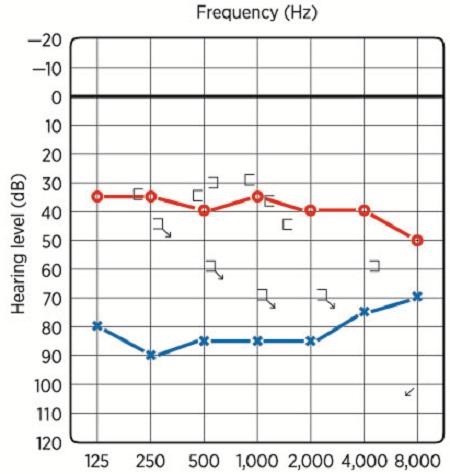
Figure 9. Audiogram for Case 1.
Due to her reluctance to trial hearing aids and the asymmetry between the hearing loss in the left and right ears, it was decided to let the patient wear a combination device (Widex mind440) on her right ear only during the trial period. Counseling was administered according to the TRT protocol (Henry et al., 2007). At the first follow-up visit after a month, she described fractal music as a comfortable listening experience and said that her anxiety was reduced. Logged data showed that she had been using the device throughout the day. After 3 months, she was coping well with her tinnitus even without the device, and her THI score had dramatically improved from 96 to 12. After five months, she began to use the amplification-only program. After six months, the amplification-only program was used more than the fractal music program, and her THI score remained low at 18. The patient’s usage pattern is summarized in Table 3.
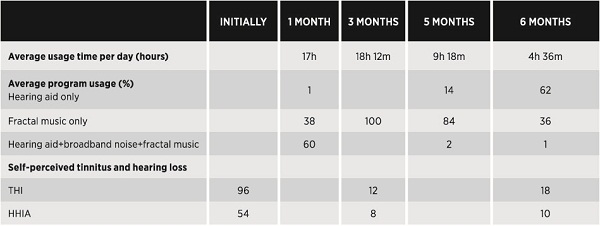
Table 3. Usage pattern and self-perceived tinnitus and hearing loss for Case 1.
Case 2
Patient 2 was a 67-year-old female who had been suffering from severe tinnitus in her left ear for more than a year. She had sought treatment at eight different clinics, and had tried a variety of therapies, but had experienced no improvement. At her initial visit, her THI score was measured at 66, and she was diagnosed with sensorineural hearing loss with an average hearing level of 47.5 dB in the right and 53.8 dB in the left ear (Figure 10). It was a typical case of presbyacusis, and hearing aids were considered. The patient rejected the suggestion of wearing hearing aids, but her tinnitus was so distressing that she was willing to try a combination device (Widex mind) as a TRT sound therapy device for her left ear.
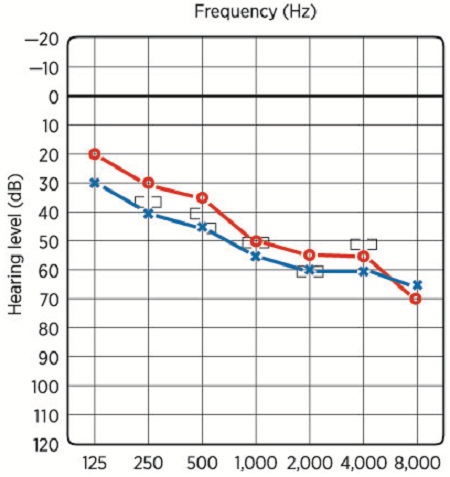
Figure 10. Audiogram for Case 2.
Initially, three program options were included in the hearing aid: hearing aid only, hearing aid + broadband noise, and broadband noise only. However, the patient complained that she was annoyed with the broadband noise already after two weeks. The broadband noise combinations were then replaced with a hearing aid + fractal music, and a fractal music-only option. An assessment of the patient’s usage pattern in the subsequent treatment period of 2.5 months revealed that she used the hearing aid + fractal music option the most. Her average daily hearing aid usage time had also increased substantially. Her THI score had improved to 50 after the three months, and the patient reported that the tinnitus had not bothered her so severely. The patient’s usage pattern is summarized in Table 4.
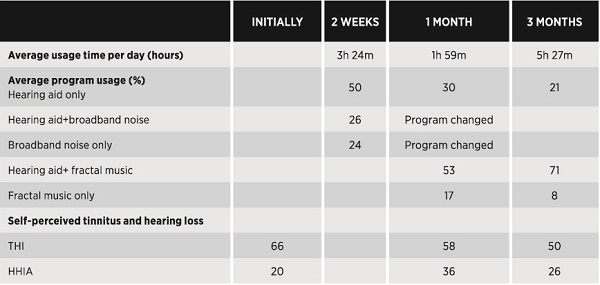
Table 4. Usage pattern and self-perceived tinnitus and hearing loss for Case 2. The broadband noise options were replaced with fractal music options after two weeks.
Conclusions
As the sound has to be listened to for prolonged periods of time, the TRT protocol prescribes the use of neutral stimuli that facilitate passive listening and do not evoke a strong emotional response in patients, such as broadband noise or conventional hearing aid amplification. Although not prohibited in TRT, music is not generally recommended, since it may invoke a strong emotional response and attract attention (Jastreboff & Hazell, 2004). However, a good effect was obtained when using the fractal music available in the Widex CLEAR, mind440, and mind220 combination devices within a TRT treatment framework. Improvements in THI scores were observed after six months in 92% of the patients who used fractal music as sound therapy. The improvements were significant (20 points or more) in 62% of the patients. Our results indicate that some patients will eventually tire of the music, which suggests that patients should be given several Zen tunes or advised to use their preferred Zen style in combination with other stimuli.
The results obtained in the present study suggest that a combination device offering flexible program combinations with conventional amplification, broadband noise and fractal music is an optimal choice for hearing-impaired patients with high THI scores. Moreover, the data logging function makes it possible to monitor the patient’s use of the different sound stimuli options in a trial period and choose the appropriate TRT device (conventional hearing aid, simple broadband noise generator, or combination device) on the basis of the patient’s usage pattern.
As illustrated by the cases reported, a flexible combination of sound stimuli is particularly useful in difficult cases where TRT with conventional sound therapy in the form of broadband noise or conventional hearing aid amplification may not always produce the desired effect. The two cases also illustrate how a combination device is sometimes effective, not only in reducing the negative effects of tinnitus, but also as a way of introducing amplification to reluctant hearing aid candidates.
References
Henry, J. A., Trune, D., R., Robb, M. J., & Jastreboff, P. J. (2007). Tinnitus retraining therapy: Clinical guidelines. San Diego: Plural Publishing.
Hertzfeld, M., & Kuk, F. (2011). A clinician's experience with using fractal music for tinnitus management. Hearing Review 18(11), 50-55.
Jastreboff, P. J. (2011). Tinnitus retraining therapy. In A. R. Møller, B. Langguth, D. DeRidder, & T. Kleinjung (Eds.), Textbook of tinnitus, pp. 575-596. New York: Springer.
Jastreboff, P. J., & Hazell, J. W. P. (2004). Tinnitus retraining therapy: An implementation of the neurophysiological model of tinnitus. Cambridge: CUP.
Kuk, F., Peeters, H., & Lau, C. (2010). The efficacy of fractal music employed in hearing aids for tinnitus management. Hearing Review, 17(10), 32 – 42.
Newman, C. W., Jacobson G. P., Spitzer J. B. (1996). Development of the Tinnitus Handicap Inventory. Archives of Otolaryngology – Head and Neck Surgery, 122(2), 143-148.
Newman, C. W., Sandridge, S. A., & Jacobson, G. P. (1998). Psychometric adequacy of the Tinnitus Handicap Inventory (THI) for evaluating treatment outcome. Journal of the American Academy of Audiology, 9(2), 153-160.
Newman, C.W., Weinstein, B. E., Jacobson, G. P. & Hug, G. A. (1990). The hearing handicap inventory for adults: Psychometric adequacy and audiometric correlates. Ear & Hearing, 11 (6), 430-433.
Sweetow, R. W., & Henderson, S. J. (2010). Effects of acoustical stimuli delivered through hearing aids on tinnitus. Journal of the American Academy of Audiology, 21(7), 461-473.
Sweetow, R. W., & Jeppesen, A. M. K. (2012). A new integrated program for tinnitus patient management: Widex Zen therapy. Hearing Review, 19(7), 20-26.
Widex A/S. (2012). Widex zen therapy: managing the effects of tinnitus. Lynge, Denmark: Widex A/S.
Zigmond, A. S., & Snaith, R. P. (1983). The Hospital Anxiety And Depression Scale. Acta Psychiatrica Scandinavica, 67, 361-70.
Cite this content as:
Sekiya, Y., Takahashi, M., Kabaya, K., Murakami, S., Yoshioka, M. (2013, March). Using fractal music as sound therapy in TRT treatment. AudiologyOnline, Article #11623. Retrieved from https://www.audiologyonline.com/
